ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Pulmonary and Critical Care Specialist, Interventional Pulmonologist, Good Samaritan Hospital, SSM Health, USA.
Pulmonary and Critical Care Specialist, Interventional Pulmonologist, Good Samaritan Hospital, SSM Health, USA.
Tel: 618-899-4000, Fax 618-242-8967;
Email: abdulmonam.ali@ssmhealth.com
Received : Jan 13, 2025,
Accepted : Feb 19, 2025
Published : Feb 26, 2025,
Archived : www.jclinmedcasereports.com
Background: Pneumatosis Cystoides Intestinalis (PCI) is a rare condition characterized by gas-filled cysts within the intestinal wall. While often benign, it can mimic life-threatening conditions such as ischemic or necrotizing colitis. This case report describes a patient with PCI in the setting of acute COPD exacerbation, highlighting the diagnostic and management challenges.
Case presentation: A 67-year-old male with severe COPD (Gold Stage IV) and a 45-pack-year smoking history presented with acute respiratory failure requiring mechanical ventilation. During his ICU stay, he developed mild abdominal distension, and imaging revealed pneumatosis coli involving the cecum and ascending colon. Given the absence of peritoneal signs, normal lactic acid levels, and stable clinical condition, a diagnosis of PCI was considered. The patient was managed conservatively with bowel rest, close monitoring, and optimization of his respiratory status. He recovered without surgical intervention and was successfully extubated, later discharged to short-term rehabilitation.
Conclusion: This case underscores the importance of recognizing PCI as a benign cause of pneumatosis coli in critically ill patients, avoiding unnecessary surgical intervention. Early diagnosis and conservative management are key to improving outcomes in such cases.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Ali A (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Pneumatosis Cystoides Intestinalis (PCI) is a rare condition characterized by the presence of gas-filled cysts within the submucosa or subserosa of the intestinal wall. While often asymptomatic or associated with mild gastrointestinal symptoms, PCI can mimic more serious conditions such as ischemic or necrotizing colitis, necessitating careful diagnostic evaluation [1,2].
PCI is typically associated with conditions that increase intraluminal pressure or disrupt mucosal integrity, such as Chronic Obstructive Pulmonary Disease (COPD), mechanical ventilation, or steroid use [3]. In critically ill patients, the distinction between benign PCI and life-threatening Pneumatosis Intestinalis (PI) is crucial, as the latter often requires urgent surgical intervention [4].
This case report describes a 67-year-old male with severe COPD who developed PCI during an acute exacerbation requiring mechanical ventilation. The case highlights the diagnostic challenges, the importance of conservative management, and the need for a multidisciplinary approach in managing such complex cases.
Patient information
A 67-year-old Caucasian male with severe COPD (Gold Stage IV) and a 45-pack-year smoking history presented to the emergency room with worsening shortness of breath and wheezing of three days’ duration. He denied chest or abdominal pain.
Clinical findings
On examination, the patient was tachypneic, on 6 liters/minute of oxygen via nasal cannula, with an SpO2 of 90%. Chest auscultation revealed diminished air entry bilaterally with bilateral expiratory rhonchi. The abdominal exam was soft with positive bowel sounds.
Initial management
The patient was initially managed with nebulized bronchodilators, systemic steroids, and empiric antibiotics. His ABG showed decompensated acute on chronic respiratory acidosis, hence, he was started on noninvasive positive-pressure ventilatory support with dexmedetomidine drip to manage agitation.
Diagnostic workup
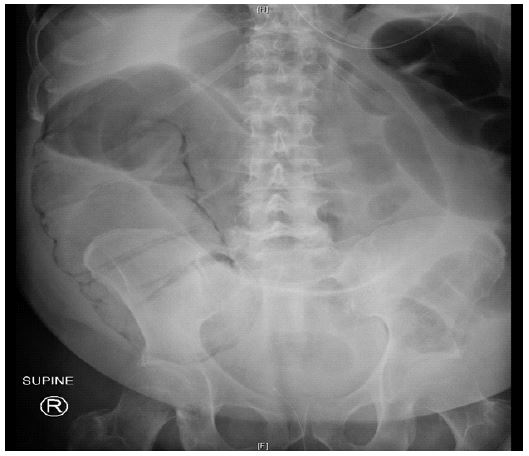
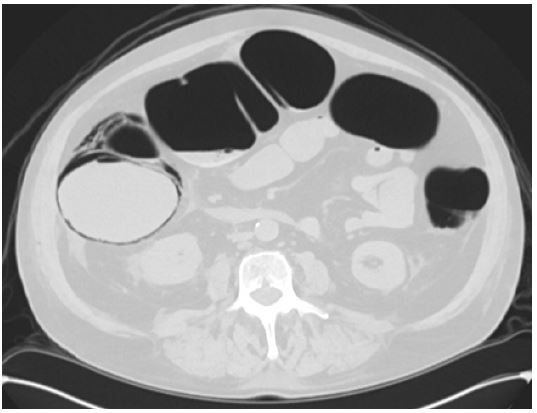
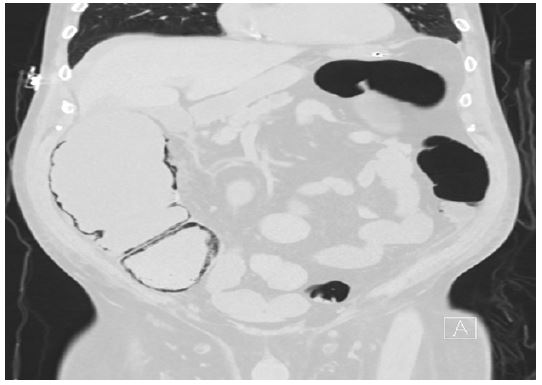
• Imaging: Chest X-ray showed hyperinflation without acute infiltrates. CT scan revealed pneumatosis coli involving the cecum and ascending colon, with no evidence of perforation or free air.
• Laboratory findings: Normal troponin levels, normal lactic acid (0.75 mmol/L), mildly elevated white blood cell count (14,000/μL), and extended respiratory viral panel (influenza, RSV, SARS-CoV-2) was negative. Blood and sputum cultures were collected.
Hospital course
Patient was admitted to medical ICU. Despite initial management, the patient’s respiratory status deteriorated, necessitating intubation and mechanical ventilation. During his ICU stay, his cultures remained negative, he developed high tube feeding residuals, mild abdominal distension without peritoneal signs. Repeat lactic acid was normal. Abdominal x-ray, CT abdomen and pelvis showed pneumatosis in the wall of the cecum and ascending colon. In context of his clinical findings, the patient was managed conservatively with bowel rest, close monitoring, and optimization of his respiratory status.
Outcome
The patient showed gradual improvement, was successfully extubated, and was later discharged to a short-term rehabilitation facility for further physical and respiratory therapy.
This case highlights the diagnostic and management challenges of PCI in a critically ill patient with acute COPD exacerbation. PCI is often asymptomatic or associated with mild gastrointestinal symptoms, making it a diagnostic challenge in the ICU setting [1,2].
The absence of peritoneal signs, normal lactic acid levels, and imaging findings without evidence of perforation or free air supported the diagnosis of PCI in this case. The mildly elevated white blood cell count was likely multifactorial, secondary to the COPD exacerbation, systemic inflammation, and steroid use [3,4].
Conservative management, including bowel rest and close monitoring, is the cornerstone of PCI treatment, particularly in the absence of concerning clinical or imaging features [5]. This case underscores the importance of avoiding unnecessary surgical intervention in patients with PCI, as timely recognition and conservative management can lead to favorable outcomes.
Pneumatosis Cystoides Intestinalis (PCI) is a rare, benign condition that can mimic more serious causes of pneumatosis coli. In this case, the patient’s clinical and imaging findings were consistent with PCI, and he was successfully managed conservatively without surgical intervention. This case highlights the importance of considering PCI in the differential diagnosis of pneumatosis coli, particularly in critically ill patients, to avoid unnecessary surgical procedures.