ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Department of Clinical and Experimental Medicine, UOC Neonatal and Pediatric Intensive Care, University Hospital of Messina, Italy.
2Department of Anaesthesia and Intensive Care, University Hospital of Messina, Italy.
Department of Clinical and Experimental Medicine, UOC Neonatal and Pediatric Intensive Care, University Hospital of Messina, Italy.
Email: rossella.morello@studenti.unime.it
Received : Feb 01, 2025,
Accepted : Mar 04, 2025
Published : Mar 11, 2025,
Archived : www.jclinmedcasereports.com
Background: Halogenated anesthetics, including sevoflurane and desflurane, are frequently utilized in pediatric anesthesia. The Anaconda® system has notably enhanced the administration of inhaled sedation in intensive care settings, demonstrating efficacy in the management of severe conditions such as refractory ARDS, ECMO patients, and those with challenging sedation requirements. Although primarily indicated for anesthetic purposes, there are anecdotal reports indicating the potential utility of these agents in the treatment of refractory status epilepticus, including in pediatric populations.
Case presentation: We present the case of a two-year and four-month-old female patient with a history of Leigh syndrome, a rare neurodegenerative disorder predominantly affecting infants and young children, who was admitted to the pediatric intensive care unit for severe respiratory failure. Despite sedation, the patient experienced refractory seizures during her hospitalization. Following a review of anecdotal case reports in the medical literature, inhaled anesthetics were administered via the Anaconda® System. This intervention resulted in clinical improvement.
Conclusion: Through this case report, we highlight the potential role of anesthetic agents as a therapeutic option for refractory epilepsy in patients with underlying metabolic disorders, particularly when conventional therapies have been ineffective.
Keywords: Halogenated anesthetics; Sevoflurane; Desflurane; AnaConda system; Refractory status epilepticus; Leigh syndrome; PICU.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rossella M (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Halogenated anesthetics, including sevoflurane and desflurane, are widely used in pediatric anesthesia. Sevoflurane is particularly favored for its smooth induction, rapid emergence, and broad therapeutic range. While generally well-tolerated, it may lead to cardiovascular side effects at high doses [1].
The Anaconda® system has notably expanded the use of inhaled sedation in intensive care, demonstrating efficacy in managing critical conditions such as refractory ARDS, ECMO patients, and those with challenging sedation needs [2-4]. Although limited, anecdotal reports in the literature suggest a potential role for inhaled anesthetics in treating refractory Status Epilepticus (SE) [6]. SE is considered refractory if first- or second-line Antiepileptic Drugs (AEDs) fail to control seizures, and it is classified as Super-Refractory Status Epilepticus (SRSE) if seizures persist for more than 24 hours despite the administration of general anesthesia [7]. Refractory status epilepticus can occur in patients with metabolic disorders, such as Leigh syndrome, a rare and severe neurodegenerative condition primarily affecting infants and young children. In this case report, we describe the successful use of sevoflurane administered via the Anaconda® system in a young patient with Leigh syndrome and intractable seizures.
A two-year and four-month-old female patient with a history of Leigh syndrome due to an MT-ATP6 gene mutation was admitted to the Pediatric Intensive Care Unit (PICU) with a Glasgow Coma Scale (GCS) score of 8, tachypnea, and oxygen dependency. Vital signs were as follows: Heart Rate (HR) 125 beats/min, Respiratory Rate (RR) ~38 breaths/min, oxygen saturation (SpO2) 89%, and Non-Invasive Blood Pressure (NIBP) 100/60 mmHg. The patient had a Percutaneous Endoscopic Gastrostomy (PEG) tube and a urinary catheter, indicating a history of chronic illness. Pulmonary auscultation revealed diffuse rhonchi, suggestive of significant airway secretions.
Immediate management included endotracheal intubation for airway protection and mechanical ventilation. A central venous catheter was inserted for medication administration and Central Venous Pressure (CVP) monitoring, and an arterial catheter was placed for invasive blood pressure monitoring.
Despite sedation, the patient experienced continuous bilateral asymmetrical focal seizures. Continuous Electroencephalography (EEG) monitoring confirmed the presence of bilateral focal occipital seizures. Prior to admission, the patient had been receiving clonazepam and vigabatrin for refractory epilepsy.
To exclude viral encephalitis as a potential cause of seizures, a lumbar puncture was performed, and Cerebrospinal Fluid (CSF) was analyzed using a FilmArray panel. Viral encephalitis was excluded within a few hours. CSF analysis for organic acids, amino acids, and lactate revealed abnormalities, confirming a metabolic etiology.
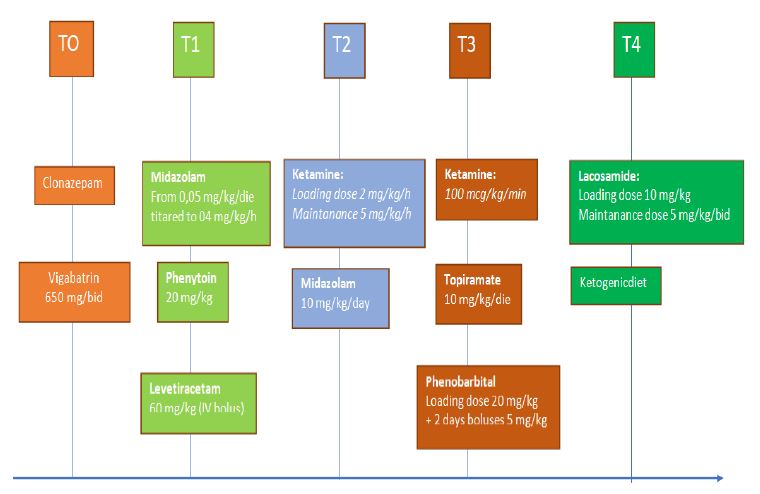
A continuous infusion of midazolam was initiated at a rate of 0.05 mg/kg/h and titrated to 0.4 mg/kg/h, providing partial seizure control. In accordance with protocol, phenytoin was administered at a dose of 20 mg/kg. Given the lack of response to treatment, a bolus of levetiracetam was administered at a dose of 60 mg/kg intravenously. Subsequently, a ketamine infusion was started with a loading dose of 2 mg/kg, followed by a maintenance dose of up to 5 mg/kg/h. Ketamine was co-administered with topiramate (10 mg/kg/day) via PEG.
As ketamine’s efficacy waned, phenobarbital was introduced. An initial bolus of 20 mg/kg was administered, followed by two daily boluses of 5 mg/kg. Systemic topiramate was continued at a dose of 10 mg/kg/day.
Given the ineffectiveness of these anticonvulsants and the exhaustion of standard therapies, lacosamide, an anticonvulsant used for refractory epilepsy, was initiated. It was administered as an initial bolus of 10 mg/kg, followed by maintenance doses of 5 mg/kg twice daily. Concurrently, a ketogenic diet was initiated as a non-pharmacological treatment for refractory epilepsy (Table 1). Despite these therapeutic adjustments, the frequency of seizures decreased but did not cease after more than 15 days of hospitalization.
The subsequent therapeutic approach involved using inhaled anesthetic vapors for sedation in the PICU via the Anaconda® system. The Anaconda vaporizer was set to a flow rate of 25 ml/h, corresponding to a 2% sevoflurane concentration. This approach significantly reduced the seizure burden. However, it induced hemodynamic instability, necessitating the initiation of norepinephrine infusion to maintain adequate blood pressure. The treatment was discontinued 24 hours later.
Leigh syndrome is a rare and severe neurodegenerative disorder primarily affecting infants and young children. It is a common manifestation of mitochondrial disease in the pediatric population. Diagnosis typically involves three key components: neuroimaging, neurological symptoms, and biochemical abnormalities. Neuroimaging studies often reveal symmetrical lesions in the brainstem and/or basal ganglia. Neurological symptoms may include developmental delay or regression, hypotonia, ataxia, dystonia, and ophthalmoplegia. Elevated lactate levels in blood or Cerebrospinal Fluid (CSF), indicative of impaired energy metabolism, are a frequent biochemical finding [7]
The clinical presentation of Leigh syndrome is highly heterogeneous. Symptoms can range from mild to severe and may encompass neurological, cardiac, hepatic, renal, and gastrointestinal manifestations. Onset typically occurs in early childhood, especially in cases associated with the MT-ATP6 mutation, as illustrated in our case [ref.]. Disease progression can be rapid and fatal, with many patients succumbing to the disease before the age of three [8].
Epilepsy is a common neurological manifestation of mitochondrial diseases affecting the central nervous system. As demonstrated by Sunho Lee et al., a significant proportion of patients with Leigh syndrome (14/25) experience seizures. The seizure spectrum in Leigh syndrome is broad, ranging from focal to generalized seizures. Despite the use of multiple Anti-Epileptic Drugs (AEDs) and specialized diets such as the ketogenic diet, many patients continue to experience recurrent seizures. These findings highlight the challenges in managing epilepsy in Leigh syndrome and emphasize the importance of individualized and multidisciplinary care [7].
Our patient, with a history of epilepsy previously treated with clonazepam and vigabatrin, had partial seizure control. During PICU admission, despite aggressive medical management, including multiple anti-seizure medications, the child continued to experience severe, uncontrollable seizures.
Refractory Status Epilepticus (RSE) and Super-Refractory Status Epilepticus (SRSE) pose significant therapeutic challenges. When first- and second-line AEDs fail to control seizures, coma induction with anesthetic agents becomes the primary treatment strategy. The choice of anesthetic agent is often individualized, with midazolam, barbiturates, and propofol commonly used. Midazolam, a fast-acting benzodiazepine, enhances the action of GABA on GABA-A receptors in the Central Nervous System (CNS) and is used to achieve electrographic/clinical seizure cessation or burst suppression. If midazolam fails to control seizures, barbiturates are typically used as second-line agents. Barbiturates, including pentobarbital and thiopental, exert their effects through GABAergic enhancement and NMDA receptor antagonism.
Propofol, while effective in controlling seizures, can be particularly risky for patients with mitochondrial disorders, as it may precipitate Propofol Infusion Syndrome (PRIS), a serious complication leading to multi-organ dysfunction, as highlighted by Josef Finsterer et al. [9]. Therefore, alternative sedative agents, such as ketamine, may be considered for these patients.
Ketamine, an NMDA receptor antagonist, has been proposed as a potential treatment for refractory status epilepticus. By reducing excessive neuronal excitation and preventing glutamate-induced neurotoxicity, ketamine offers a therapeutic strategy for RSE/SRSE. The ketogenic diet, a well-established dietary therapy for drug-resistant epilepsy, offers an adjunctive therapeutic option. By altering brain metabolism, the ketogenic diet can reduce seizure frequency and may serve as an adjunct to pharmacological treatments [10-11].
In our case, the patient received a combination of conventional and unconventional therapies, including benzodiazepines, barbiturates, ketamine, and other anti-seizure medications, without significant benefit. Additionally, a ketogenic diet was implemented as a non-pharmacological approach to reduce seizure frequency.
Inhaled anesthetics, such as isoflurane and desflurane, are often considered a last-line therapy for refractory status epilepticus. These agents exert their anti-seizure effects by enhancing GABAergic inhibition and inhibiting glutamatergic excitation. They can effectively induce burst-suppression patterns on Electroencephalogram (EEG), which can be titrated to achieve the desired level of sedation. However, the widespread use of inhaled anesthetics in the ICU has been limited by technical complexities and high costs.
The Anaconda® system is an innovative device designed to address these challenges. It simplifies the delivery of inhaled anesthetics and reduces resource utilization by using existing critical care ventilators, common syringe pumps, and gas monitors to administer precise doses of isoflurane or sevoflurane [10].
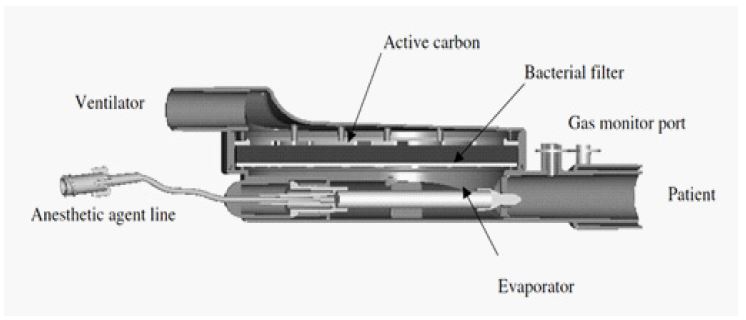
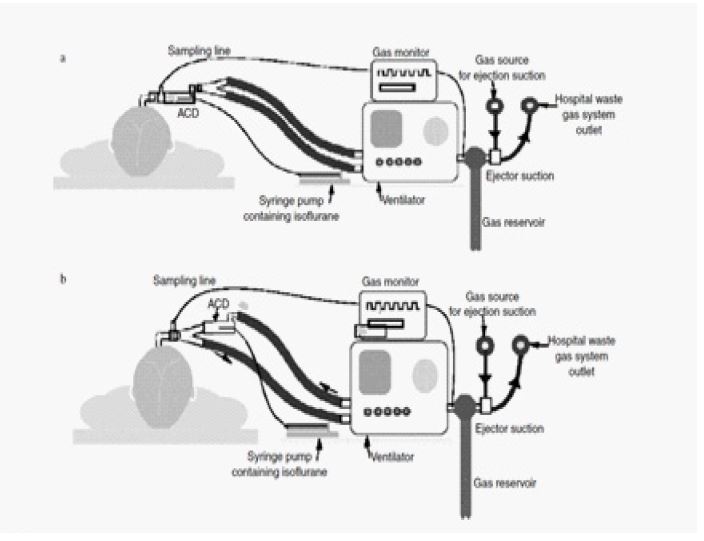
The device (Figure 1) is a modified heat and moisture exchanger that can be integrated into the breathing circuit in two configurations: either connected to the Y-piece (Figure 2a) or positioned in the inspiratory limb (Figure 2b). The system facilitates the delivery of isoflurane or sevoflurane via a syringe pump. The gas is vaporized within the AnaConDa and incorporated into the inspired gas mixture. When positioned at the Y-piece, approximately 90% of exhaled gas is captured by a carbon filter within the device and re-inspired by the patient due to concentration gradients. This rebreathing mechanism significantly reduces isoflurane consumption, limiting it to the amount metabolized and a small portion released to the scavenging system. Alternatively, when placed in the inspiratory limb, the rebreathing function is lost, but this configuration avoids the addition of dead space at the Y-piece, which may benefit smaller patients [5-12].
In our case, the AnaConDa device was set to a flow rate of 25 ml/h, corresponding to a vaporizer setting of 2% sevoflurane.
The treatment outlined above successfully achieved the desired outcome in our patient, resulting in a significant reduction in seizure frequency, as documented by EEG, after 24 hours of administration. Notably, the use of sevoflurane was associated with potential hemodynamic effects, including hypotension that was refractory to fluid resuscitation. In such instances, vasopressor support, specifically norepinephrine, may be required, as observed in our patient.
As highlighted in the literature, inhalational anesthetic agents can play a crucial role in cases where other treatment modalities have failed. In our case, multiple attempts to sedate the young patient and control seizure frequency were either ineffective or only partially successful. This case suggests that inhaled anesthetics, administered via the Anaconda system, may represent a valuable therapeutic option for refractory status epilepticus, particularly in patients with Leigh syndrome.
The use of the Anaconda® (Anaesthetic Conserving Device) is not standard practice in Intensive Care Units (ICUs), especially in pediatric settings. However, in this instance, its efficacy was immediate, with the desired dose being reached within minutes. Despite the rapid and notable therapeutic effect, it is essential to consider the potential for adverse events, which should be carefully weighed against the benefits when considering this approach in clinical practice.
A more in-depth prospective investigation is necessary to evaluate the efficacy and safety of inhalational anesthetics in the management of Refractory Status Epilepticus (RSE) in pediatric patients. Such studies are crucial to better understand the potential therapeutic benefits and risks associated with these agents in this specific patient population.
Author declarations: Consent for publication.
Written informed consent was obtained from the patient for publication of this case report.
Competing interests: All the authors have read and understood the journal policy on the declaration of interest and declare that we have no competing interests.
Author’s contributions: All authors read and approved the final manuscript.