ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Department of Pulmonary and Critical Care Medicine, Corewell Health West, Grand Rapids, Michigan, USA.
2College of Human Medicine, Michigan State University, Grand Rapids, Michigan, USA.
3Department of Internal Medicine, Corewell Health West, Grand Rapids, Michigan, USA.
Department of Pulmonary and Critical Care Medicine, Corewell Health West, Grand Rapids, Michigan, USA.
Tel: +1(929) 507 9325;
Email: cheeyao.lim@corewellhealth.org
Received : April 12, 2025,
Accepted : May 14, 2025
Published : May 21, 2025,
Archived : www.jclinmedcasereports.com
We present a rare case of coil migration to the right heart following embolization of a spontaneous portosystemic venous shunt in an 87-year-old man with multiple comorbidities, including coronary artery disease, valve replacement, chronic right-sided heart failure, and atrial fibrillation. The patient initially underwent coiling for a large intrahepatic shunt but developed coil migration to the right ventricle, confirmed by non-contrast CT of the thorax. Fluoroscopy revealed the coil was embedded in the anterior wall of the right ventricle. Due to the patient’s high surgical risk and the coil’s stable position, conservative management was pursued. He remained hemodynamically stable, and no clinical deterioration occurred as a result of the migration.
Intravascular coil migration is a rare but serious complication of embolization procedures. While retrieval is generally recommended, this case underscores the importance of individualized management decisions, particularly in elderly patients with significant comorbidities. This report adds to the limited literature on this topic and emphasizes the role of multimodal imaging and multidisciplinary risk assessment in managing such complications.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Lim CY (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
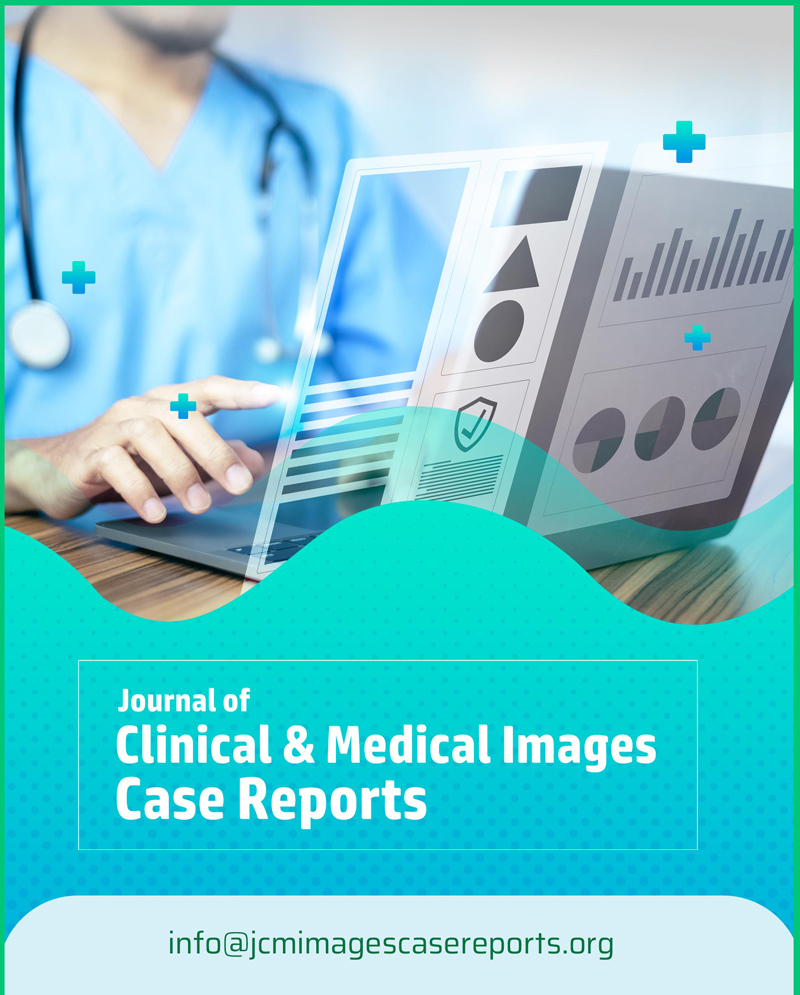
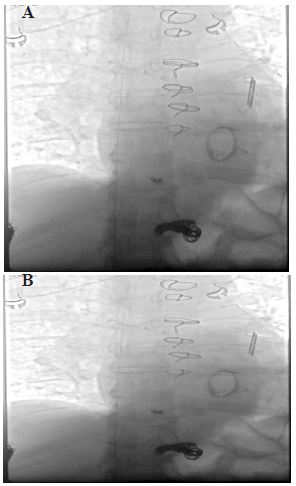
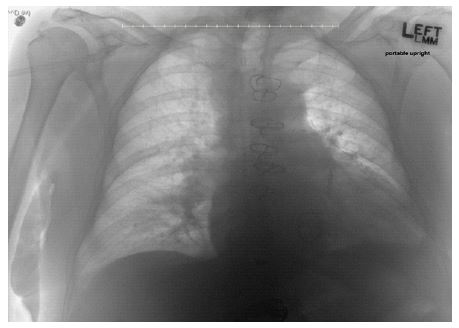
An 87-year-old man with an underlying history of coronary artery disease post coronary artery bypass graft, mitral valve replacement, moderate aortic stenosis, chronic right-sided heart failure, bronchial asthma, and atrial fibrillation initially presented with dyspnea and features of right heart strain on transthoracic echocardiogram. This was believed to be related to the development of intrahepatic porto-hepatic venous shunts from spontaneous portosystemic venous malformations, the largest of which was 4 centimeters. He had initially presented to the interventional radiology department for shunt embolization via coiling. The procedure was complicated by one of the coils migrating to the right ventricle. CT Thorax was performed to as sess the location of coil migration, and it revealed the coil to be deep in the anterior aspect of the right ventricle (Figure 1).
An attempt was made to retrieve the coil via fluoroscopy by interventional radiologist but was unsuccessful. The coil was adherent to the anterior right ventricular wall, and it was felt to be at a low risk of further embolization. Due to the patient’s advanced age and comorbidities, no further attempts were made at retrieving the coil, given the risk-benefit ratio. There was no family or personal history of Hereditary Hemorrhagic Telangiectasia (HHT) nor any symptoms or clinical signs suggestive of HHT. However, given the spontaneous development of portosystemic shunt and hematuria, he was referred to the genetics outpatient clinic for further testing.

Intrahepatic portosystemic shunt is a rare condition defined as communication between the intrahepatic portal vein and systemic veins. It is associated with portal hypertension. It can be treated conservatively or via transcatheter embolization [1]. The procedure’s migration of coil embolization is a rare complication, with few prior reports of coil embolization to the right heart or pulmonary vasculature available in the literature [2,3]. We described a case of coil migration to the right heart and ultimately treated it conservatively.
Percutaneous embolization of the hepatic veins is well documented as a treatment for portosystemic shunts. Reports of intravascular migration of embolization coils are rare events. A few case reports describe coil embolization to the pulmonary artery, resulting in pulmonary infarct [4]. To our knowledge, this is the first report of coil migration in the setting of attempted embolization of hepatic portosystemic venous shunting. In the vast majority of cases, foreign bodies of the right heart result from migration from various pieces of medical/non-medical devices and rarely result in direct penetration [5].
Foreign bodies in the right side of the heart pose potential complications, including infective endocarditis, thrombosis, pulmonary embolism, pulmonary infarct, erosion, perforation and tamponade, arrhythmia or conduction disturbances, paradoxical embolization, and in rare circumstances, possible cardiopulmonary arrest [5]. Experts recommend early removal of intracardiac foreign bodies to prevent complications, even if clinically silent. Methods of removal can be a percutaneous approach under IR guidance or via open heart surgery. In our case, the patient was considered to be at high surgical risk given his multiple comorbid conditions and could not be anticoagulated because of the complication of hematuria. He was, therefore, managed conservatively, and this has been described in the literature in the case of small and smooth foreign bodies. Tonkin et al. described two instances of coil migration to the tricuspid valve and pulmonary arteries with coil fragments in the right ventricle, which was asymptomatic and was managed conservatively [6]. In conclusion, coil migration is a rare complication of portosystemic shunt coil embolization. Failure of coil retrieval is rare, and further effort in retrieval via open heart surgery has to be weighed on a case-by-case basis based on the patient’s comorbidities and associated risks.
The patient was asymptomatic as a result of the coil migration and had no clinical deterioration. His hospitalization was complicated by acute kidney injury, hematuria from cystitis, hypoxia post procedure requiring high-setting BiPAP support in the ICU from pulmonary edema, an episode of bradycardia, which was mostly felt to be from robust vagal tone as it occurred during sleep. Cardiology was consulted and felt the bradycardia was benign, needing no further treatment. He was discharged home after 11 days of inpatient hospital stay.