ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Department of Radiology, Hospital Ibn Sina, Mohammed V University, Rabat, Morocco.
Department of Radiology, Hospital Ibn Sina, Mohammed V University, Rabat, Morocco.
Email: rania.imezirki96@gmail.com
Received : April 16, 2025,
Accepted : May 19, 2025
Published : May 26, 2025,
Archived : www.jclinmedcasereports.com
Pseudoaneurysms following aorta-femoral bypass are rare but serious complications that can lead to severe morbidity if not promptly diagnosed and managed. These pseudoaneurysms typically occur at the site of graft anastomosis, where mechanical stress or infection may compromise the vessel wall, leading to the formation of an aneurysmal sac; clinical presentations can vary from asymptomatic to fatal haemorrhagic complications. Early detection through various imaging modalities is necessary for accurate diagnosis and timely management. We herein represent the case of a 55-year-old man who presented to the emergency room with a right femoral pseudoaneurysm fistulated to the skin, secondary to an aortic-bifemoral bypass for a ruptured aneurysm operated 2 years ago.
Keywords: Pseudoaneurysm; Aorto-bifemoral bypass; Vascular surgery; Duplex ultrasound; CT angiography.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Rania I (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Pseudoaneurysms are uncommon but potentially serious complications following aortic-femoral bypass surgery. These lesions arise due to a disruption in the arterial wall, leading to blood leakage and the formation of a pulsatile hematoma contained by surrounding tissues. They are often linked to graft infection requiring debridement of infected tissue and frequently complete or partial graft removal [2]. Clinically, pseudoaneurysms typically present as a pulsatile mass, a palpable thrill, and an audible to-and-fro murmur [1], but clinical manifestations may vary from incidental findings to life-threatening presentations. Diagnosis relies on various imaging modalities, with duplex sonography at the forefront, followed by Computed Tomography Angiography (CTA) [3-5]. While the use of synthetic grafts has significantly improved outcomes in vascular surgery, the development of pseudoaneurysms remains a constant concern for surgeons with potential severe morbidity and mortality, thus the importance of timely recognition and appropriate management.
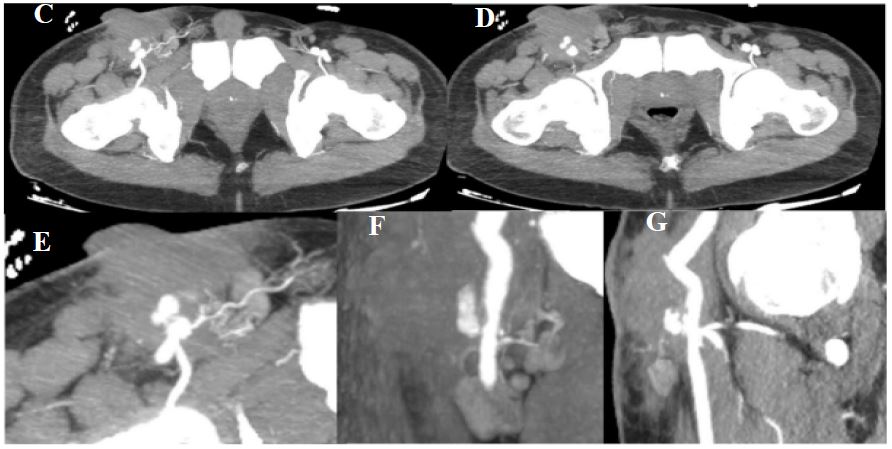
A 55-year-old patient with a history of severe psoriasis and ruptured aortic aneurysm for which he underwent an aortic-bifemoral bypass 2 years ago presented to the emergency department of our hospital with a round pulsatile mass with a palpable thrill fistulised to the skin of the right groin area (Figure 1) where he has been previously operated several times for recurrent anastomotic breakdown without notable improvement. Given the clinical presentation highly suggesting a pseudoaneurysm, a Doppler ultrasound was conducted, revealing a hypoechoic tery with “to and FRO” Doppler flow within the pseudoaneurysm, indicating blood entering and exiting the sac through a narrow neck. The additional examination performed with CTA identified a saccular pseudoaneurysm at the level of the right distal insertion of the anteriorlateral circumferential bypass, measuring 15×14 mm with a neck measuring 7×7 mm. This false aneurysm is contained within a hematoma measuring 72×56 mm (Figure 2). The patient was urgently admitted to the operating room, where he underwent surgical repair for his pseudoaneurysm. The patient is currently still hospitalised at the vascular surgery department and was put under antibiotics as well as treatment for his psoriasis flare-up.

A Pseudoaneurysm (PSA) is a pulsatile hematoma communicating with the lumen of an artery through a disruption in the arterial wall; they are most commonly found in the groin as a complication of endovascular procedures, vascular trauma or following open vascular surgery where they are usually related to graft infections [2]. The incidence of PSA varies between 0.06% and 0.18% after diagnostic interventions and 0.7% to 6.25% after therapeutic interventions [3]. Pseudoaneurysms are associated with significant morbidity and mortality closely correlated to various relevant risk factors such as female sex, older age, diabetes, arterial hypertension, peripheral arterial occlusive disease, as well as obesity [3].
Clinically, pseudoaneurysms typically present as a pulsatile mass with palpable thrill and an audible to-and-fro murmur accompanied by localised pain or tenderness [1]. Rarely, pseudoaneurysms may be asymptomatic and discovered incidentally or conversely present acutely with complications such as rupture, infection or compression leading to numbness, swelling, or oedema in the affected limb.
Radiologically, there are multiple vascular imaging modalities with relatively high sensitivity and specificity; these include duplex ultrasound, which is considered the gold standard for the diagnosis of pseudoaneurysms due to its accessibility, low cost and non-invasiveness; it allows the assessment of blood flow within the femoral veins and arteries, the pseudoaneurysm and its communicating tract [3]. It typically reveals a round anechoic or hypoechoic pulsatile mass contiguous to the artery with a “to and FRO curve” Doppler flow formed by the systolic and diastolic in- and outflow of blood from the PSA [3]. Duplex Ultrasound has a sensitivity and specificity of 94–99% and 94– 97%, respectively [3], hence allowing the diagnosis with high accuracy, but in some cases, further examination with Computed tomography and magnetic resonance angiography may be required for complex origins or retroperitoneal location [3]. On CTA, PSA presents as a well-defined, contrast-enhancing outpouching adjacent to the arterial wall, connected to the parent artery through a narrow neck; it may have a saccular or fusiform shape and appear as a contrast-filled cavity. PSAs could also be surrounded by hematomas or soft tissue oedema, especially in case of a recent rupture or infection.
Several conditions can mimic the clinical and radiological appearance of pseudoaneurysms; these include true aneurysms, which involve all three arterial wall layers and are usually secondary to degenerative and atherosclerotic disease. Arteriovenous Fistula may also present as a pulsatile mass but is differentiated by an arterial-to-venous flow without a sac. Hematoma can also be mistaken for a pseudoaneurysm but lacks arterial communication on imaging. Other differential diagnoses include abscess, soft tissue mass and vascular malformations. Accurate differentiation relies on a thorough clinical history, physical examination, and imaging studies.
This case is particularly noteworthy because of the unique combination of psoriasis, vascular surgery, and the occurrence of a pseudoaneurysm with skin fistulisation. Our patient’s psoriasis could have contributed to the complexity of this case, as his chronic skin condition may interfere with wound healing and increase the risk of infections, potentially leading to the fistulisation of the skin, which has complicated the clinical picture. This case underscores the importance of considering underlying comorbidities and their impact on postoperative outcomes when managing vascular complications.
On a therapeutic level, pseudoaneurysms have long been treated effectively by open surgery up until the late 90s [3], but due to the multitude of severe intra and postoperative complications such as infections, healing disorders, bleeding, thrombosis and oedema [3] other surgical options have been preferred such as peripheral bypass, reconstruction using grafts, and ligation of involved vessels [4,5]. Alternative therapies have also been used since; these include Ultrasound-Guided Compression Therapy and thrombin injection or endovascular repair [3]. In some cases of small, asymptomatic and uncomplicated pseudoaneurysms in patients who do not need anticoagulation, therapeutic abstention and close monitoring may be considered [1]. In our case, due to the recurrent anastomotic breakdown and the patient’s underlying chronic skin condition, open surgical repair was the preferred therapeutic method.
Pseudoaneurysms following aorto-bifemoral bypass represent a rare but serious complication that requires prompt recognition and management. Their development is often influenced by graft integrity, surgical technique, and patient comorbidities, including infection or systemic conditions; advanced imaging modalities, particularly CTA and duplex ultrasound, play a pivotal role in diagnosis and treatment planning. Management strategies depend on the size, location, and symptoms of pseudoaneurysms, with options including surgical repair, endovascular intervention, or, in select cases, conservative management with close monitoring. Early detection and timely intervention are crucial in minimising morbidity and mortality, emphasising the importance of vigilant postoperative surveillance in patients undergoing aorto-bifemoral bypass. This highlights the need for a multidisciplinary approach to optimise outcomes in these complex cases.