ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Department of Pediatrics, Division of General Pediatrics, Ege University Faculty of Medicine, Izmir 35100, Turkey.
2Department of Pediatrics, Division of Social Pediatrics, Ege University Faculty of Medicine, Izmir 35100, Turkey.
Department of Pediatrics, Division of General Pediatrics, Ege University Faculty of Medicine, Izmir 35100, Turkey.
Phone: +90 232 390 12 69;
Email: sule.gokce@yahoo.com
Received : Jun 20, 2025,
Accepted : Jul 07, 2025
Published : Jul 14, 2025,
Archived : www.jclinmedcasereports.com
Septo-Optic Dysplasia (SOD) is a rare neurodevelopmental disorder characterized by a triad of optic nerve hypoplasia, absence of the septum pellucidum, and hypothalamo-pituitary dysfunction. It was first described in 1941 and has been associated with young maternal age, maternal drug use, viral infections, and genetic predisposition. SOD-plus syndrome extends this classic triad by including associated malformations of cortical development. This means that in addition to the core features of SOD, individuals with SOD-plus also have abnormalities in the outer layer of the brain (cerebral cortex). This case report presents a 53-day-old female infant diagnosed with SOD-plus who exhibited rotatory nystagmus. This article aims to highlight that early diagnosis and a multidisciplinary treatment approach can improve patients’ quality of life.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Gökçe Ş (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Septo-Optic Dysplasia (SOD), also known as de Morsier syndrome, is primarily defined by the triad of optic nerve hypoplasia and/or optic chiasm hypoplasia, absence of the septum pellucidum or corpus callosum dysgenesis, and with or without hypothalamo-pituitary dysfunction. The heterogeneous developmental disorder is not fully understood, but it is believed to be associated with genetic predisposition (mutations in genes such as HESX1, SOX2, OTX2, and SOX3), young maternal age, maternal drug use (e.g., alcohol, cocaine, or anticonvulsants), prenatal viral infections etc. [1]. The incidence of SOD is estimated to be between 1 in 10,000 and 1 in 50,000 live births. However, the actual prevalence may be higher due to underdiagnosis, especially in cases with mild or incomplete features. It occurs sporadically in most cases, but genetic factors have been implicated in some familial cases [2]. The clinical manifestations include a wide range of features such as hypoglycemia, hyperbilirubinemia, nystagmus, visual impairment, psychomotor retardation, seizures, and cognitive impairments in the early neonatal and infant period. Progressive visual impairment is the most typical finding, with severe optic nerve hypoplasia, oftenleading to blindness, being the main cause of visual deficits [3]. Optic nerve involvement occurs due to maldevelopment or underdevelopment of the optic nerves, which are responsible for transmitting visual information from the eyes to the brain in SOD. This can result in optic nerve hypoplasia, where the optic nerves are smaller than usual or poorly formed. The exact mechanisms behind this maldevelopment are not fully understood but are believed to involve disruptions during early brain development, specifically in the hypothalamus and septum pellucidum, which are structures that influence the development of the optic nerves. Genetic factors and environmental influences during pregnancy may also contribute to optic nerve abnormalities in SOD. Due to optic nerve hypoplasia, visualacuity varies from normal to no lightperception depending on the integrityof the papillomacular nerve fi bre bundleof the retina. As a result, visual impairment or blindness can occur, depending on the severity of optic nerve involvement [4]. Hypopituitarism is observed in 62–80% of individuals with SOD, with growth hormone deficiency being the most prevalent endocrine disturbance. However, deficiencies in Thyroid-Stimulating Hormone (TSH), Adrenocorticotropic Hormone (ACTH), and Gonadotropin-Releasing Hormone (GnRH) may also be present. Midlinebrain malformations, observed in approximately 60% of cases, include the absence of the septum pellucidum and/or agenesis of the corpus callosum. Septo-optic Dysplasia-plus syndrome goes beyond the typical triad of Septo-optic Dysplasia (SOD) by also featuring related malformations of cortical development. This means that, alongside the classic SOD symptoms, individuals with SOD-plus exhibit abnormalities in the brain’s outer layer, the cerebral cortex. The most frequently observed cortical malformation is schizencephaly, characterized by slits or clefts in one or both brain hemispheres. Other cortical abnormalities, such as polymicrogyria or heterotopic gray matter, can also occur. Cognitive impairments, along with neurological manifestations such as developmental delays, seizures, and cerebral palsy, are frequently reported. Other associated findings encompass diabetes insipidus, sleep disturbances, autism spectrum disorder, precocious puberty, obesity, thermoregulatory dysfunctions, anosmia, sensorineural hearing loss, as well as various cardiac and limb anomalies [5].
We describe a case of binocular nystagmus with a history of perinatal hypoglycemia, prolonged jaundice, optic nerve hypoplasia, and midline brain abnormalities (interventricular septum aplasia, optic chiasm hypoplasia, ectopic neurohypophysis), along with associated panhypopituitarism. This case highlights the complexity of the condition and underscores the need for comprehensive diagnostic evaluation and multidisciplinary management to address both the visual and neurological aspects of the disorder.
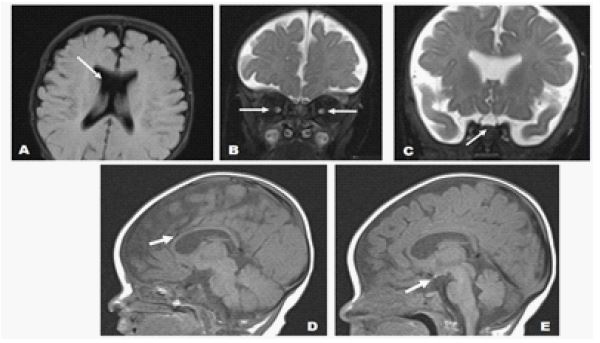
A 53-day-old female infant was referred to our hospital with complaints of rotatory nystagmus and prolonged jaundice. The prenatal period was uneventful, and the mother had no systemic illnesses during pregnancy. Delivery occurred spontaneously at 40+5 weeks of gestation, with a birth weight of 3700 g. On postnatal day 1, the infant developed hypoglycemia and was monitored in the neonatal intensive care unit for 11 days. Following discharge, she attended regular outpatient follow-ups. On examination, the infant appeared icteric, exhibited poor eye tracking, and demonstrated searching nystagmus. Neurological evaluation revealed normal muscle tone. A 2/6 systolic murmur was detected on cardiovascular examination, while other systemic evaluations were within normal limits. Laboratory investigations revealed the following results: total bilirubin: 11.8 mg/dL, direct bilirubin: 0.62 mg/dL. Given the suspicion of hypopituitarism, hormonal analysis was performed, showing free T4: 0.71 ng/dL (low), TSH: 6 ìIU/mL (mildly elevated), ACTH: 24.9 pg/mL (normal), cortisol: 0.75 ìg/dL (low), and prolactin: 91.1 ng/mL (elevated). Echocardiography identified a small apical muscular Ventricular Septal Defect (VSD) and a 2 mm Atrial Septal Defect (ASD) with left-to-right shunting. Ophthalmological examination revealed optic nerve hypoplasia, which was considered the primary cause of the visual impairment. Transfontanel ultrasound showed a corpus callosum thickness of 2 mm, suggestive of hypoplasia. The septum pellucidum was absent, and a single ventricle anomaly was noted. Cranial Magnetic Resonance Imaging (MRI) findings included bilateral optic nerve and optic chiasm hypoplasia, absence of the septum pellucidum, and an ectopic neurohypophysis, Supporting the Diagnosis of SOD (Figure 1). To investigate potential genetic etiologies, Whole Exome Sequencing (WES) was performed on the patient’s blood sample. Comprehensive analysis of known SOD-associated genes (e.g., HESX1, SOX2, OTX2, SOX3) and other relevant neurodevelopmental genes did not identify any pathogenic or likely pathogenic variants. This finding indicates a lack of identifiable genetic correlation with known mutations in this particular case. Based on clinical, laboratory, and radiological evaluations, the patient was diagnosed with septo-optic dysplasia, and a multidisciplinary follow-up plan was established. Endocrinological support therapy was initiated due to hypopituitarism, and the patient was closely monitored for growth hormone deficiency, adrenal insufficiency, and other endocrine dysfunctions. The family was thoroughly informed about the risk of vision loss associated with optic nerve hypoplasia, and appropriate interventions were recommended to support visual development.
Septo-Optic Dysplasia (SOD) is a complex syndrome that poses diagnostic challenges due to the variability and rarity of its clinical manifestations. Not all classical features are present in every case, and the clinical presentation may differ based on genetic and environmental factors. Therefore, a comprehensive, multidisciplinary approach is essential for an accurate diagnosis. While genetic testing and radiological imaging serve as gold-standard diagnostic tools, hormonal profiling plays a pivotal role in identifying associated endocrine dysfunctions. The core triad of SOD includes optic nerve hypoplasia, absence of the septum pellucidum, and hypothalamo-pituitary dysfunction; however, these features do not always coexist [1]. Patients are at risk for vision loss and neurodevelopmental disorders, making endocrinological and neurological follow-up crucial. Vision loss due to optic nerve hypoplasia significantly impacts quality of life, necessitating early intervention and visual rehabilitation. The management of SOD is primarily symptomatic. Hormonal replacement therapies are required to address endocrine dysfunctions such as hypopituitarism, often necessitating lifelong monitoring. Supportive therapies, including glasses, low-vision aids, and visual rehabilitation programs, are recommended for those with optic nerve hypoplasia. Furthermore, early referral to special education and rehabilitation programs is essential for addressing potential developmental delays.
This case really emphasizes that Septo-Optic Dysplasia (SOD) is a rare condition with a wide range of symptoms. It highlights how crucial early diagnosis and a multidisciplinary treatment approach are for better patient outcomes. The absence of identified genetic mutations in this case further emphasizes the complex and multifactorial nature of SOD. Specifically, it’s important to consider SOD in infants who have persistent nystagmus and hypoglycemia, even if they don’t have clear facial abnormalities. Multidisciplinary follow-up is essential to prevent both physical and neurodevelopmental complications. Managing SOD is complex, requiring expert care at every stage, and long-term follow-up is highly recommended.