ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Gastroenterology Institute, Rambam Health Care Campus, Israel.
Gastroenterology Institute, Rambam Health Care Campus, Israel.
Email: eisahag158@gmail.com
Received : Jun 23, 2025,
Accepted : Jul 07, 2025
Published : Jul 14, 2025,
Archived : www.jclinmedcasereports.com
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Hag E (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Percutaneous Endoscopic Gastrostomy (PEG) tubes require timely replacement to prevent complications like degradation, migration, and buried bumper syndrome. Prolonged retention poses significant risks. We report a case of PEG tube migration after over a decade of use without replacement.
A female patient underwent uncomplicated PEG placement in February 2012 for nutritional support due to cognitive decline and dysphagia. No plan for routine replacement was documented.
Over the next decade, despite multiple hospitalizations (for urosepsis in 2014/2015, aspiration pneumonia in 2021) and documented home care visits confirming feeding via the PEG (2015-2022), the tube was never assessed for replacement. Its presence was noted occasionally, once with luminal clots (Jan 2015), but no action was taken. An early attempt at replacement failed due to lack of a legal guardian. The patient became bedridden and demented, with a DNR status. The family reported trimming the external tube over time.
In 2023, 11 years post-insertion, she presented with suspected internal PEG migration. The external stoma was clean, but the tube was absent. Abdominal CT located the tube in the duodenum.
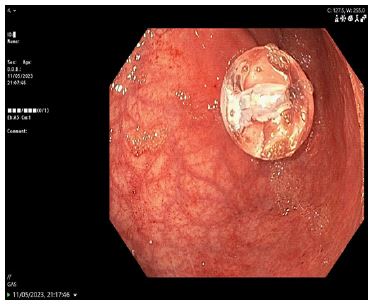
A temporary Foley catheter secured the tract. Subsequent endoscopy did not visualize the tube in the duodenum but found the gastrostomy device within the stomach (Figure 1). A new 14F replacement tube was inserted. The duodenal component seen on CT was presumed likely to pass spontaneously (Figure 2), and the patient was monitored for obstruction.

This case exemplifies complications from neglecting long-term PEG tube management. The 11-year retention period grossly exceeds recommended replacement intervals (6-12 months initially) [1], leading to presumed material fatigue and migration.
Failures in care coordination across multiple hospitalizations and home care settings contributed to this preventable event, despite the patient’s known dependence on the device. The discrepancy between CT (duodenal location) and endoscopy (gastric location) may suggest intermittent migration or fragmentation. Standard guidelines emphasize regular inspection and planned replacement, which were critically lacking here, potentially compounded by the patient’s complex medical and social status.
This case underscores the importance of regular evaluation and timely replacement of PEG tubes. The lack of clearly defined follow-up responsibilities and scheduled maintenance led to a cascade of complications, highlighting a critical gap in the long- term management of enteral feeding devices in high-risk patients.