ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*Department of General Surgery A21, Charles Nicolle Hospital, Faculty of Medicine of Tunis, Tunisia.
Department of General Surgery A21, Charles Nicolle Hospital, Faculty of Medicine of Tunis, Tunisia.
Email: docteur.yassine123@gmail.com
Received : Jun 25, 2025,
Accepted : Jul 10, 2025
Published : Jul 17, 2025,
Archived : www.jclinmedcasereports.com
Keywords: Hydatid cyst; Pancreas; Hydatid serology; Surgery; Resection.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Yassine T (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
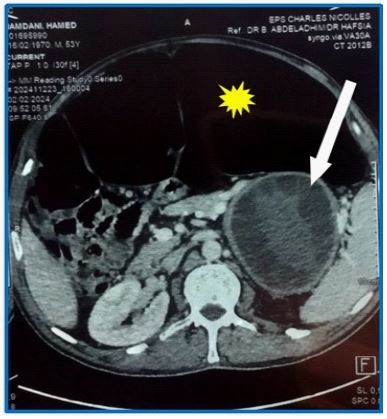
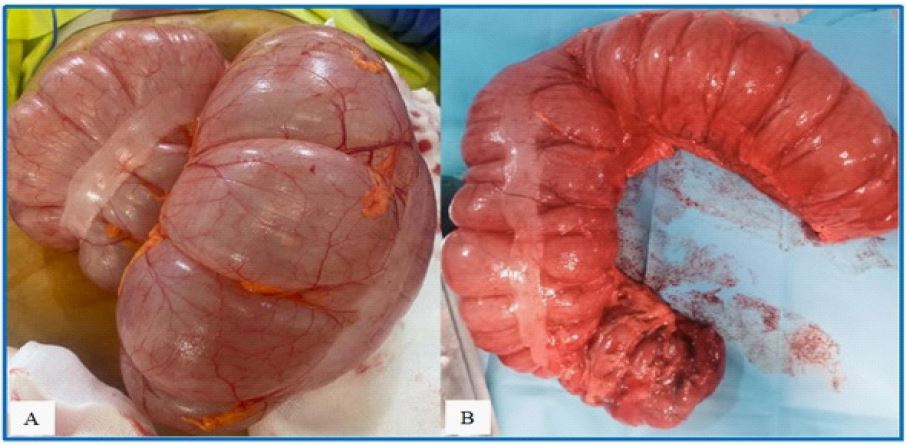
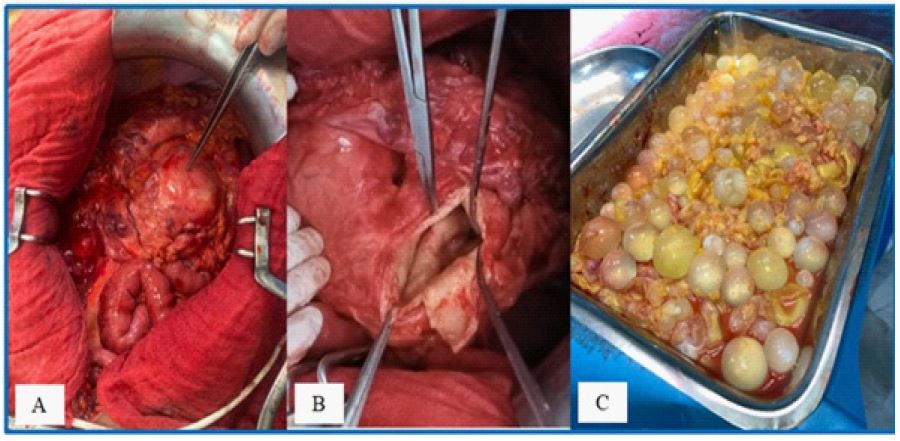
We report the case of a 54-year-old man with a history of sigmoidectomy for volvulus who developed chronic colonic dilatation requiring repeated colonic exsufflation. Abdominal CT imaging revealed pancolonic distension and a large (11 × 9 × 13 cm) multilocular pancreatic tail cyst causing segmental portal hypertension (Figure 1). Hydatid serology was positive, suggesting a diagnosis of a pancreatic hydatid cyst. The patient underwent an exploratory laparotomy. Intraoperatively, the entire colon was distended (Figure 2A), and a well-defined cys t ic lesion was found in the pancreatic tail, which was densely adherent to the spleen and associated with collateral venous circulation (Figure 3A). We performed a subtotal colectomy (Figure 2B) without immediate restoration of intestinal continu ity, combined with partial resection of the pancreatic hydatid cyst (Figure 3B). The cyst contents, consisting of non-infected multivesicular fluid (Figure 3C), were completely evacuated. A drain was placed in the residual cavity. Postoperative recovery was uncomplicated, with no recurrence at 6-month follow-up.
Hydatid disease remains a significant public health concern in Tunisia [1]. Although the liver is the predominant site of infec tion, isolated pancreatic involvement is extremely uncommon, representing only 0.14-2% of systemic echinococcosis cases [2].
Due to their rarity, pancreatic hydatid cysts are often misdi agnosed as other cystic pancreatic lesions. Preoperative diagno sis requires multimodal imaging (contrast-enhanced CT, MRI, or ultrasound) combined with hydatid serology [2,3].
Surgical treatment is mandatory, with the approach (radi cal or conservative) depending on the cyst’s location relative to the mesenteric-portal pedicle, anatomical relationships, and complications [3]. In our case, the cyst’s proximity to the spleen, presence of segmental portal hypertension, and need for concurrent colectomy necessitated a conservative surgical approach.