ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Department of Gastroenterology, Istinye University Liv Bahcesehir Hospital, Istanbul, Turkey.
2Department of Internal Medicine and Division of Gastroenterology, Texas Tech University Health Sciences Center, Lubbock, Texas,
USA.
Department of Internal Medicine and Division of Gastroenterology, Texas Tech University Health Sciences Center, Lubbock, Texas,
USA.
Email: Hakan. Akin@ttuhsc.edu
Received : Jul 03, 2025,
Accepted : Aug 05, 2025
Published : Aug 12, 2025,
Archived : www.jclinmedcasereports.com
A case of cholangitis caused by live Fasciola hepatica is presented. The patient, diagnosed with cholangitis, was treated with 10 mg/kg oral triclabendazole after the parasite was removed with Endoscopy Retrograde Cholangiopancreatography (ERCP).
Keywords: Fasciola hepatica; Cholangitis; ERCP; Jaundice.
Abbreviations: ERCP: Endoscopic Retrograde Cholangiopancreatography; MRCP: Magnetic Resonance Cholangi-Opancreatography; FH: Fasciola Hepatica; CBD: Common Bile Duct; WBC: White Blood Cells; GGT: Gammaglutamyl Transpeptidase; AST: Aspartate Aminotransferase; ALT: Alanine Aminotransferase; ALP: Alkaline phosphatase; FDA: Food and Drug Administration; WHO: World Health Organization.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Akin H (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Fasciola Hepatica (FH) is a parasite of the leafworm family, commonly seen in domestic animals and rarely found in humans as intermediate hosts. Most of the FH cases reported in the literature are from South America, Eastern Europe, Africa, China, Australia, and the Middle East [1]. Humans may be accidental hosts of FH by the consumption of contaminated water or vegetables. The parasite can cause biliary tract obstruction, cholangitis, cholecystitis, and pancreatitis [2]. Parasite larvae penetrate the intestinal wall and enter the peritoneal cavity [3]. Adult parasites can cause obstructive jaundice, similar to gallstones, and may lead to cholangiocarcinoma [4]. The living parasite in the Common Bile Duct (CBD) is rarely found, as the parasite usually lives in the gallbladder and the thin branches of the biliary tree [5].
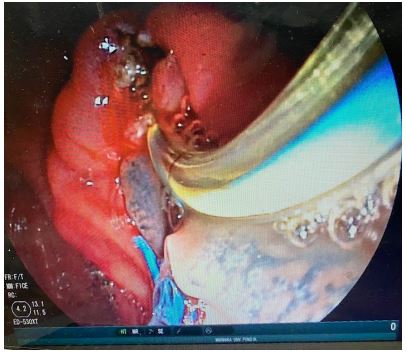
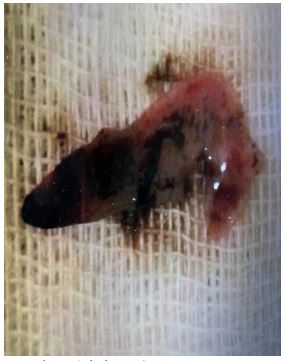
A 58-year-old female patient was admitted to our Gastroenterology Clinic with complaints of severe right upper abdominal pain, nausea, and jaundice. She had right upper abdominal pain for a month, worsening at night, and jaundice for the past week. The patient lived in Eastern Anatolia (FH endemic area) and had a history of eating vegetables from her garden. On physical examination, the patient was jaundiced, and the right upper quadrant of the abdomen was tender to palpation. The patient’s hemogram showed a white blood cell count of 12000/mm3 and 18% eosinophilia in the peripheral smear. Her hemoglobin and platelet values were normal. Biochemical parameters: total bilirubin 7 mg/dl, direct bilirubin 5 mg/dl, aspartate Aminotransferase (AST) 35 IU/L, Alanine Aminotransferase (ALT) 65 IU/L, GammaGlutamyl Transpeptidase (GGT) 190 IU/L, Alkaline Phosphatase (ALP) 245 IU/L. Abdominal ultrasound revealed moderate bile duct dilatation. Magnetic Resonance Cholangiopancreatography (MRCP) showed possible distal stenosis of the common bile duct. Endoscopic retrograde cholangiopancreatography (ERCP) was performed for diagnosis and treatment. During the ERCP procedure, live parasites were spilled into the duodenal cavity (Figure 1). The parasite was removed with a basket, and an antiparasitic drug (triclabendazole) was applied (Figure 2). Immediately after the parasite was removed from the bile duct, the patient’s pain in the right upper quadrant subsided.
Fasciola hepatica is a leaf-shaped parasite usually found in domestic animals, such as sheep. When an individual accidentally ingests the parasite from raw vegetables or contaminated water, the parasite larvae may survive gastric acid and enzymes, penetrate the intestinal wall, and enter the peritoneal cavity, where they invade the liver [2]. FH may cause obstructive jaundice and is a risk factor for cholangiocarcinoma [4]. Human fascioliasis has two phases: an acute phase resulting from liver invasion and a chronic phase characterized by the presence of parasites in the bile ducts [6]. Untreated fasciolosis can lead to recurrent attacks of cholangitis and secondary biliary cirrhosis [7]. The patient’s history of living in an endemic area and eating inadequately washed vegetables may provide diagnostic clues. The patient presented to us with jaundice and right upper abdominal pain. It is well established that ERCP is utilized in both diagnosis and treatment [8]. ERCP, in addition to facilitating diagnosis, provides the opportunity to remove parasites from the common bile duct lumen after sphincterotomy. In this case, both diagnosis and treatment were achieved with ERCP. Triclabendazole is the drug of choice for human fascioliasis. The drug was approved for human use by the U.S. Food and Drug Administration (FDA) in 2019. The recommended dose by WHO and the US FDA is 10 mg/kg [9]. We administered triclabendazole to the patient at recommended doses.
FH may cause obstructive jaundice or predispose the patient to cholelithiasis, a risk factor for cholangiocarcinoma. This parasite is an important differential diagnosis of obstructive jaundice in countries with a high prevalence of fasciolosis. ERCP contributes significantly to the diagnosis and treatment of FH.