ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Department of Microbiology, St. Xavier’s College, Mother Teresa Sarani, Kolkata, India.
2Peerless Hospitex Hospital and Research Center Limited, Kolkata, India.
Peerless Hospitex Hospital and Research Center Limited, Kolkata, India.
Email: : drsatdas@hotmail.com
Received : Jul 14, 2025,
Accepted : Aug 17, 2025
Published : Aug 24, 2025,
Archived : www.jclinmedcasereports.com
Mucormycosis was an important complication in COVID-19 particularly during Delta strain of SARS-CoV-2 infections. In this manuscript we report six cases of mucormycosis in patients presenting with COVID-19, along with diabetes mellitus, and renal complications. All patients exhibited typical mucormycosis symptoms alongside various underlying conditions, including diabetes and renal disease. Diagnostic imaging and laboratory tests confirmed the presence of mucormycosis. The primary treatment consisted of antifungal therapies and the management of several underlying health issues. Mucormycosis poses a significant threat to patients with COVID-19, diabetes, and renal disease. Early diagnosis and aggressive treatment are critical for improving patient outcomes.
Keywords: Mucormycosis; COVID-19; SARS-CoV-2; Diabetes mellitus; Renal diseases.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Das S (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
The impact of SARS-CoV-2 infection on the incidence and severity of mucormycosis has been significant during the second wave of the COVID-19 pandemic when infections were mainly due to Delta strain of the virus. Mucormycosis, commonly referred to as black fungus, is a rare but aggressive fungal infection caused by moulds belonging to the order Mucorales, which are found in soil, decaying organic matter, and animal dung [1,2]. While typically harmless to healthy individuals, it can become life-threatening in immunocompromised patients. Several interrelated factors contribute to the heightened risk of mucormycosis in COVID-19 patients. COVID-19 infection triggers a cytokine storm, especially an increase in Interleukin-6 (IL-6), which raises ferritin levels and disrupts iron metabolism, leading to excess free iron. This promotes the formation of Reactive Oxygen Species (ROS), fostering an environment conducive to fungal growth. In parallel, COVID-19 may cause acute hyperglycaemia, new-onset diabetes, hypoxia, lymphopenia, reduced CD4+/CD8+ T cells, and metabolic acidosis—all of which compromise immune defences [3,4]. The use of corticosteroids in managing severe COVID-19 can worsen hyperglycaemia, suppress immune function, and increase ferritin and ROS levels, further enhancing susceptibility to fungal infections. Patients with pre-existing diabetes are at particular risk, as chronic hyperglycaemia and Diabetic Ketoacidosis (DKA) create acidic environments that facilitate fungal proliferation. During DKA, the endothelial receptor GRP78 and fungal CotH proteins are upregulated, promoting adhesion and tissue invasion by Mucorales [5]. Without prompt antifungal therapy, the fungal load can double within hours, making early diagnosis critical. During the pandemic, the rapid progression of mucormycosis significantly increased mortality rates, especially in patients with comorbidities such as diabetes mellitus, renal disease, and haematological malignancies like leukaemia and lymphoma. In addition to individuals with COVID-19 and diabetes, several other groups are particularly vulnerable to mucormycosis due to compromised immune defences [6,7]. These include patients undergo ing chemotherapy or those who have received organ or stem cell transplants, as their immune systems are often significantly suppressed with prolonged neutropenia. Long-term corticosteroid therapy can impair the immune response and elevate blood sugar levels, creating favourable conditions for fungal growth. Patients with chronic kidney disease often have weakened immunity and may undergo treatments that increase susceptibility to opportunistic infections. Rhino-Cerebral Mucormycosis primarily affects the sinuses, eyes, and brain and is most commonly seen in individuals with uncontrolled diabetes or Diabetic Ketoacidosis (DKA). Early symptoms include nasal congestion, black discharge from the nose, facial pain or swelling, vision disturbances, and altered mental status. If not treated promptly, the infection can progress rapidly and may be fatal [8]. Pulmonary Mucormycosis involvement is typically seen in patients with weakened immune systems, such as those undergoing chemotherapy or organ transplantation. The infection targets the lungs, causing symptoms like fever, persistent cough, chest pain, shortness of breath, and haemoptysis. This form can closely resemble other respiratory infections like tuberculosis or aspergillosis, making diagnosis challenging [9]. A rare but serious form, gastrointestinal mucormycosis is mainly observed in premature infants and critically ill adults. It commonly affects the stomach or intestines and presents with symptoms such as abdominal pain, vomiting, gastrointestinal bleeding, and abdominal distension. Without timely intervention, the condition carries a high risk of mortality [10]. Cutaneous mucormycosis occurs when fungal spores enter the body through breaks in the skin, such as cuts, burns, surgical wounds, or trauma. It manifests as redness, swelling, pain, ulceration, and black necrotic lesions at the site of infection. If not treated effectively, the fungus can spread to deeper tissues and potentially become systemic [11]. The most severe form of the disease, disseminated mucormycosis occurs when the infection spreads through the bloodstream to multiple organs, including the brain, heart, spleen, and skin. Symptoms vary depending on the organs affected and often indicate severe systemic involvement. This form is associated with a very poor prognosis and requires urgent, aggressive treatment [12]. Absidia produces relatively small sporangia that are round to pear-shaped and are held on a distinctive funnel-shaped structure called an apophysis. This feature differentiates Absidia from the genera Mucor and Rhizomucor, which possess larger, globose sporangia lacking an apophysis. There are 21 known species in the Absidia genus, and most of them live in soil. Among them, Absidia corymbifera is a recognized opportunistic human pathogen, capable of causing various forms of zygomycosis, including pulmonary, rhinocerebral, disseminated, Central Nervous System (CNS), and cutaneous infections [13]. The genus Cunninghamella is characterized by rapidly growing colonies that range in colour from white to grey. These colonies produce straight, upright, branching sporangiophores. At their tips, the sporangiophores terminate in globose (round) or pyriform (pear-shaped) vesicles. These vesicles give rise to multiple single-celled, round to oval sporangiola, which form on swollen projections. The sporangiola may have smooth or spiny (echinulate) walls. In addition, chlamydospores and zygospores may also be present. Colonies grow very quickly, appearing white initially and gradually turning dark grey and powdery as sporangiola form. Sporangiophores can reach up to 20 µm in width and may be straight with either solitary or verticillate (whorled) branches. Terminal vesicles are sub globose to pyriform and can measure up to 40 µm in diameter, while lateral vesicles range from 10–30 µm. Sporangiola are typically globose (7–11 µm) or ellipsoidal (9–13×6–10 µm), with surfaces that may be warty (verrucose) or slightly spiny (short-echinulate). Individually, they are hyaline, but in large numbers, they appear brownish. The optimal growth temperature is between 25–30°C, with a maximum up to 50°C. These fungi are primarily soil-dwelling organisms found in Mediterranean and subtropical regions, and are rarely isolated from temperate climates. Among the seven species in the genus, only Cunninghamella bertholletiae is known to infect humans and animals, often following trauma or in immunocompromised individuals [14]. Rhizopus is a genus of common fungi that function primarily as saprophytes, feeding on decaying plant material, though some species can also act as specialized parasites of animals. These fungi are widely distributed in nature and thrive on a broad range of organic matter, including ripe fruits and vegetables, jellies, syrups, bread, leather, peanuts, and tobacco. Rhizopus species are multicellular and form filamentous structures. Some members of this genus are opportunistic pathogens in humans and can cause a severe and often fatal infection known as mucormycosis, particularly in immunocompromised individuals. The genus comprises at least eight recognized species. Morphologically, Rhizopus fungi grow as fast-spreading, filamentous hyphae that are coenocytic— meaning they lack cross-walls and form a continuous cytoplasmic mass. They reproduce through both asexual and sexual means: In asexual reproduction, spores are produced within spherical structures called sporangia, which are supported by a large, swollen base known as the apophysate columella. These sporangia are held on long stalks called sporangiophores, which arise among root-like structures known as rhizoids and two compatible hyphae fuse to form a thick-walled, dark zygospore. When conditions are favourable, the zygospore germinates and gives rise to a new colony that is genetically distinct from the parent strains. Notable species and their uses or effects include Rhizopus oligosporus widely used in food biotechnology, particularly in the production of tempeh, a traditional fermented soybean product common in Southeast Asia. Rhizopus oryzae – employed in the fermentation of alcoholic beverages in various parts of Asia and Africa. Rhizopus stolonifera (commonly known as black bread mould) – A frequent cause of post-harvest fruit rot, affecting crops like strawberries, tomatoes, and sweet potatoes. Industrially, it plays a role in the commercial production of fumaric acid and cortisone [15,16]. This study presents a total of six cases of mucormycosis, each associated with underlying conditions such as COVID-19, diabetes mellitus, and renal disease. In the first case, the patient tested positive for COVID-19 and had a history of hypertension. This individual experienced a rare and severe complication in the form of Renal Allograft Rupture (RAR), which further complicated the clinical course of mucormycosis. The second case involved a patient diagnosed with Diabetes Mellitus and chronic renal disease; conditions known to compromise immunity and predispose individuals to invasive fungal infections. The third case shared a similar medical background, as the patient also had diabetes and renal disease, but was additionally COVID-19 positive, highlighting the combined immunosuppressive effect of the virus and comorbidities. The remaining fourth, fifth, and sixth cases were likewise found in patients with Diabetes Mellitus and renal dysfunction, indicating a consistent pattern of underlying risk factors across the case series. The patients’ ages ranged from 45 to 65 years, representing a middle-aged to elderly demographic typically at greater risk for severe outcomes. This study aims to analyse the occurrence and clinical management of mucormycosis in patients with overlapping conditions—specifically COVID-19 infection, diabetes mellitus, and renal disease.
With permission from Institutional Ethical Committee keeping all the patients anonymous retrospective data were analysed in six cases.
DNA extraction protocol (tissue): First, the tissue sample was cut and ground thoroughly. Then, 20 μl of QIAGEN protease was pipetted into a 1.5 ml microcentrifuge tube. After that, 180 μl of ATL buffer was added to the same tube. The mixture was vortexed and incubated at 56°C for 10 minutes. Following incubation, 200 μl of buffer AL was added to the sample, mixed by pulse vortexing for 15 seconds, and incubated again at 70°C for 10 minutes. To remove any drops from the inside of the lid, the tube was briefly centrifuged.
Next, 200 μl of ethanol was added to the sample, mixed by pulse vortexing for 15 seconds, and the tube was centrifuged again to remove lid condensation. Afterward, 5 μl of Internal Control (IC) was added to a 2 ml microcentrifuge tube. The tube was then capped and centrifuged at 8000 rpm for 1 minute.
The 2 ml spin column was placed into a clean 2 ml collection tube, and the tube containing the filtrate was discarded. The spin column was carefully opened, and 500 μl of Buffer AW1 was added without wetting the rim. The column was capped and centrifuged at 8000 rpm for 1 minute. The spin column was then transferred to a new 2 ml collection tube, and the previous collection tube was discarded.
Subsequently, the spin column was placed into a fresh 1.5 ml microcentrifuge tube, and the previous collection tube containing the filtrate was discarded. Finally, 200 μl of Buffer AE or distilled water was carefully added to the center of the spin column membrane. After incubating at room temperature for 1 minute, the tube was centrifuged at 8000 rpm for 1 minute to elute the DNA.
Real time detection protocol
The Mucor-Genius® Real-Time PCR Kit had been validated on real-time PCR instruments such as the CFX96 and C1000 thermal cyclers, utilizing different fluorescence detection channels. For optimal detection, the HEX dye was employed for Mucorales spp., and the CY5 dye was used for the internal control (IC), with appropriate filter settings applied to their respective channels.
The real-time PCR thermal cycling program began with an initial activation and denaturation step at 95°C for 2 minutes, during which the Taq DNA polymerase was activated and the double-stranded DNA was denatured into single strands. This was followed by 45 amplification cycles, each consisting of denaturation at 94°C for 15 seconds and a combined annealing and extension step at 58°C for 60 seconds. During the latter, primers annealed to their complementary sequences, and DNA synthesis was carried out by the polymerase enzyme.
To prepare the master mix for each 25 μl reaction, 10 μl of Mucor-Genius® PCR mix, 1 μl of Taq polymerase, and 9 μl of dilution buffer were combined, making up 20 μl per reaction. This master mix was dispensed into each PCR tube or well, while the reagents were maintained on ice or a cooling block to preserve enzyme activity and prevent premature reactions.
Subsequently, 5 μl of extracted DNA containing the internal control was added to the master mix for each test sample, 5 μl of dilution buffer was added to the negative control, and 5 μl of Mucor-Genius® positive control was added to the positive control reaction. After all additions, the PCR tubes or plate were sealed, briefly centrifuged to collect contents at the bottom, and then placed into the CFX96 real-time PCR system (Bio-Rad) for analysis.
Case 1
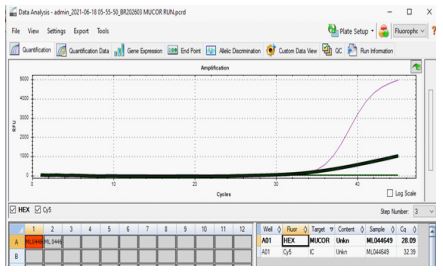
A 50 year-old male patient with a history of poorly controlled type 2 diabetes and recent recovery from moderate COVID-19 presented with facial pain, right eye swelling, black nasal discharge, and headache. On examination, he had periorbital edema, ptosis, and necrotic tissue in the nasal cavity. Imaging revealed sinus involvement with possible orbital extension. Nasal swab and KOH mount confirmed broad aseptate hyphae, and culture identified Rhizopus species, indicating rhino-orbital mucormycosis. He was promptly started on intravenous liposomal amphotericin B and underwent surgical debridement. With antifungal therapy and improved glycemic control, the patient showed gradual clinical recovery.
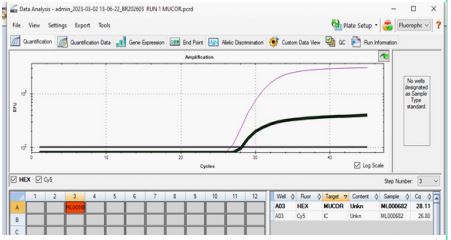
(CT) value of 28.45 in RT PCR (Figure 1) indicates a moderate fungal load. Laboratory investigations revealed a significantly elevated Total Leukocyte Count (TLC) of 18,000/mm3 , suggestive of an ongoing infection or inflammation, and a haemoglobin level of 9.4%, indicating anaemia. Based on the clinical findings and diagnostic results, the patient was started on antifungal therapy with Amphotericin-B, suspecting a possible invasive fungal infection, which is commonly seen in post-COVID-19 immunocompromised individuals, particularly with uncontrolled diabetes and a history of organ transplantation.
Case 2
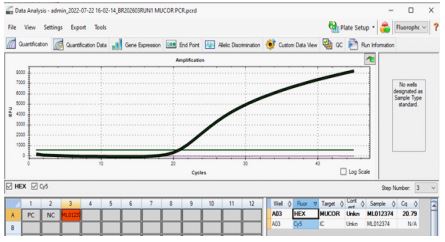
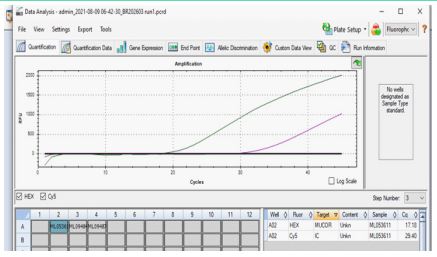
A 53-year-old male patient, recently recovered from COVID-19, with a history of uncontrolled diabetes mellitus and underlying renal disease, has tested positive for mucormycosis. Diagnostic investigations revealed a significantly elevated Total Leukocyte Count (TLC) of 25,500/mm3 , indicating a strong inflammatory or infectious response, and a haemoglobin level of 8.8%, suggestive of anaemia, while the clinical specimen, obtained as a swab from an oral ulcer, showed a low Cycle Threshold (CT) value of 20.79 (Figure 2), indicating a high fungal load and necessitating urgent medical intervention.
Case 3
We report the case of a 65-year-old female with a known history of diabetes mellitus (HbA1c: 11.2%), who had recovered from COVID-19 infection 30 days prior. Her treatment course included prolonged corticosteroid therapy. She was referred to our facility with complaints of intermittent fever, cough, respiratory distress, and required mechanical ventilation upon admission. Initial microbiological investigations, including aerobic and anaerobic bacterial and fungal cultures from blood, sputum, and urine, showed no pathogenic growth. Clinically, the patient had previously experienced pneumonia and recurrent painful aphthous ulcers on non-keratinized oral mucosa. Her condition progressed to include an arterial pseudoaneurysm and episodes of waxing and waning respiratory function.
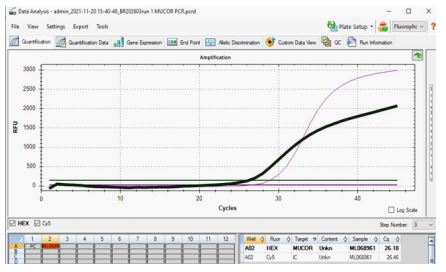

Radiological findings revealed a cavity in the left lung measuring 7 cm × 5 cm with a 5 mm thick wall. A tissue specimen collected from this cavity was sent for histopathological examination. Laboratory investigations showed a C-Reactive Protein (CRP) level of 272 mg/L and a Total Leukocyte Count (TLC) of 22,000 cells/μL. The CT (cycle threshold) value was recorded as 26.18 (Figure 3). Histopathology of the tissue biopsy from the cavity wall revealed broad, aseptate fungal hyphae consistent with Zygomycetes, demonstrated on both Grocott’s Methenamine Silver (GMS) and Periodic Acid-Schiff (PAS) stains (Figure 4). Additionally, Real-Time Pan-fungal PCR confirmed the presence of Mucorales DNA. The patient was promptly started on Liposomal Amphotericin B (L-AmB); however, despite aggressive antifungal therapy, she deteriorated rapidly and succumbed to the infection within three days of treatment initiation
Case 4
A 41-year-old male patient with a known history of post-COVID-19 infection, underlying diabetes mellitus, and a pre-existing kidney disorder was clinically diagnosed with mucormycosis, confirmed through microbiological analysis of two distinct clinical specimens. The first specimen, serum, demonstrated a cycle Threshold (CT) value of 28.09 (Figure 5), while the second specimen, sputum, showed a comparatively lower CT value of 25.2, indicating a relatively higher fungal load in the respiratory tract and signifying an active and possibly progressing infection. Further laboratory investigations revealed a markedly elevated Total leukocyte Count (TC) of 20,000, which is indicative of a significant inflammatory or infectious response, and a decreased Haemoglobin percentage (HB%) of 8.4, suggesting anaemia that may contribute to reduced oxygen-carrying capacity, tissue hypoxia, and overall physiological compromise. These haematological derangements, when combined with the patient’s comorbid conditions and immunosuppressive state due to both diabetes and renal dysfunction, place him at heightened risk for poor outcomes, underscoring the urgency for aggressive antifungal therapy, glycaemic control, and multidisciplinary management.
Case 5
A 48-year-old male with a history of poorly controlled diabetes and recent recovery from COVID-19 presented with sudden onset of right-sided facial pain, nasal blockage with blackish discharge, swelling around the right eye, and confusion. On examination, there was drooping of the eyelid (ptosis), forward displacement of the eye (proptosis), and black necrotic patches inside the nose. MRI scans revealed infection involving the ethmoid and maxillary sinuses, spread to the orbit, and early extension into the brain’s frontal lobe—indicating rhinocer ebral mucormycosis. Lab tests from nasal tissue showed broad, ribbon-like aseptate fungal hyphae, and culture confirmed Rhizopus species. The patient was diagnosed with rhinocerebral mucormycosis and promptly started on intravenous liposomal amphotericin B along with emergency surgical debridement. Blood sugar levels were strictly controlled, and with supportive care, the patient improved.
Laboratory investigations revealed a Total leukocyte Count (TC) of 16,700, while the haemoglobin level (HB%) was at 11.1%. The patient’s renal disease complicates the clinical scenario further, potentially impairing immune function and limiting the pharmacological options for antifungal treatment, thereby necessitating comprehensive and carefully monitored multidisciplinary management approach.
Case 6
A 58- year- old female patient with a medical history notable for hypertension, poorly controlled type II diabetes mellitus (HbA 1 c: 11. 6%), and chronic renal disorder was admitted with complaints of severe pain on the right side of her face and eye, accompanied by facial puffiness, eyelid swelling, and headache. Clinical examination revealed complete ophthalmoparesis on the right side, along with a history of right facial weakness, and she had also developed a low- grade fever (100°F) for 2-3 days before admission. MRI of the brain demonstrated age- related cerebral parenchymal atrophy, alongside bilateral periventricular and deep white matter ischemia, likely secondary to small vessel arteriosclerotic disease. A CT of the Paranasal Sinuses (PNS) with contrast revealed diffuse, peripherally contrast- enhancing mucosal soft tissue thickening in the right maxillary sinus extending into the right nasal cavity, with expansion of the osteomata unit, involvement of the ethmoid sinus, and erosion of the medial wall of the right orbit.
Further MRI orbit screening indicated residual mucosal thickening in the bilateral maxillary sinuses and right frontal, ethmoid, and sphenoid sinuses, along with lobulated soft tissue in the right orbit indenting the medial rectus muscle, with evidence of haemorrhage, raising the possibility of sequelae of orbital cellulitis progressing to endophthalmitis. Laboratory investigations showed a markedly elevated Total leukocyte Count (TC) of 26,500, suggesting an intense infectious or inflammatory response, and a low Haemoglobin level (HB% %) of 8.3, indicating moderate anaemia. The final diagnosis included right orbital cellulitis with maxillary sinusitis due to mucormycosis (confirmed by PCR), left hemiplegia secondary to a massive infarct in the right Middle Cerebral Artery (MCA) territory, uncontrolled type II diabetes mellitus, systemic hypertension, and chronic liver disease, all contributing to a complex and critical clinical condition requiring urgent multidisciplinary intervention.
Mucormycosis is a life-threatening opportunistic fungal infection that predominantly affects immunocompromised individuals, including those with diabetes mellitus, renal diseases, and haematological malignancies, and among its various forms, pulmonary mucormycosis represents a relatively rare but severe manifestation that is notoriously difficult to diagnose early due to non-specific clinical and radiological features and lacks uniformly effective treatment options; it is more frequently observed in patients with haematological malignancies [17,18] uncontrolled diabetes, and those undergoing immunosuppressive therapy, with diagnosis relying heavily on histopathological identification of broad, aseptate fungal hyphae in lung tissue or the detection of fungal DNA using real-time pan-fungal PCR techniques, while the emergence of COVID-19-Associated Pulmonary Mucormycosis (CAPM) has further complicated the clinical landscape, necessitating a heightened index of suspicion and often requiring bronchoscopy for definitive diagnosis [19] especially since the presence of visual necrosis is linked to poor prognosis and high mortality, and the coexistence of MultidrugResistant (MDR) bacterial infections further exacerbates outcomes, particularly in patients treated with corticosteroids during COVID-19, which significantly promotes the proliferation of Mucorales fungi, thereby making CAPM a condition that poses substantial diagnostic and therapeutic challenges in already critically ill patients [20].
The study highlights the concerning intersection of COVID-19, diabetes mellitus, and renal disease as a fertile ground for the emergence of mucormycosis, a life-threatening opportunistic fungal infection. Through six detailed case observations, the paper demonstrates that these comorbidities—especially when accompanied by immunosuppressive treatments such as corticosteroids—significantly increase vulnerability to mucormycosis.
Early diagnosis using imaging and PCR-based fungal detection, combined with aggressive antifungal therapy (e.g., Amphotericin B), is crucial for improving outcomes. Uncontrolled diabetes and renal dysfunction severely compromise immunity, elevating the risk of a poor prognosis. Multidisciplinary management is essential due to the complex, multi-system involvement in these patients. The paper emphasizes the need for heightened clinical suspicion in post-COVID patients with underlying comorbidities who present with sinus, orbital, or pulmonary symptoms. In summary, the research underscores mucormycosis as a growing threat in the post-COVID era, especially among diabetic and renal-compromised populations, and calls for vigilant diagnostic protocols and early, aggressive intervention.
Conflict of interest: There was no conflict of interest of this manuscript.
Acknowledgement: We hereby acknowledge the Managing Director, Peerless Hospitex Hospital and Research Centre, Kolkata, India, for the support and encouragement, and for providing the necessary resources for conducting this experiment.