ISSN Number
ISSN 2771-019X-

-

Impact Factor
1.2*
ISSN Number
ISSN 2771-019X
Impact Factor
1.2*1Department of Cardiology, Mount Sinai Hospital, Newyork – 10029, USA.
2Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bengaluru – 560041, India.
3Department of Cardiology, Mehta Hospitals, Chennai – 600 077, India.
4Department of Radiology, Al-Dhannah Hospital, Al Dhannah, Abu Dhabi, UAE.
5Department of Radiology, Mahadeshwara Diagnostics, Mysore, Karnataka – 570021, India.
Department of Cardiology, Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bengaluru – 560041, India.
Tel: +91-8122566969
Email: drnarendran92@gmail.com
Received : Aug 08, 2025,
Accepted : Sep 08, 2025
Published : Sep 15, 2025,
Archived : www.jclinmedcasereports.com
Fulminant myocarditis is a rare and life-threatening condition characterized by rapid hemodynamic deterioration and severe ventricular dysfunction. This report details a 33-year-old female with high-grade fever, syncope, and progression to complete heart block and ventricular arrhythmias. Despite transvenous pacing and antiarrhythmic therapy, the patient rapidly progressed to refractory cardiogenic shock and succumbed within hours due to severe left ventricular dysfunction. This case report emphasizes the need for early recognition, aggressive management, and the potential role of mechanical circulatory support in fulminant myocarditis to improve outcomes in this devastating condition.
Keywords: Fulminant myocarditis; Cardiogenic shock; Mechanical circulatory support; VA-ECMO; Ventricular arrhythmias.
Copy right Statement: Content published in the journal follows Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0). © Dhanasekaran N (2025).
Journal: The Journal of Clinical and Medical Images, Case Reports (JCMICR) is a fantastic resource for keeping up with the latest clinical advancements and for publishing case reports and clinical images related to a variety of medical illnesses.
Fulminant myocarditis represents a unique subset of acute myocarditis, marked by a dramatic clinical course and variable prognosis. Specific aetiologies, such as giant cell myocarditis, cardiac sarcoidosis, and eosinophilic myocarditis, frequently exhibit a fulminant phenotype. Due to its rapid clinical deterioration, timely and precise management is essential, but this is often challenging in resource-limited settings where advanced diagnostic and therapeutic tools, such as cardiac MRI and Mechanical Circulatory Support (MCS), may be unavailable. There is no definitive diagnostic modality; however, cardiac MRI, endomyocardial biopsy, and clinical presentation provide valuable diagnostic clues. The advent of MCS devices has significantly advanced treatment approaches, promising improved outcomes in fulminant myocarditis [1].
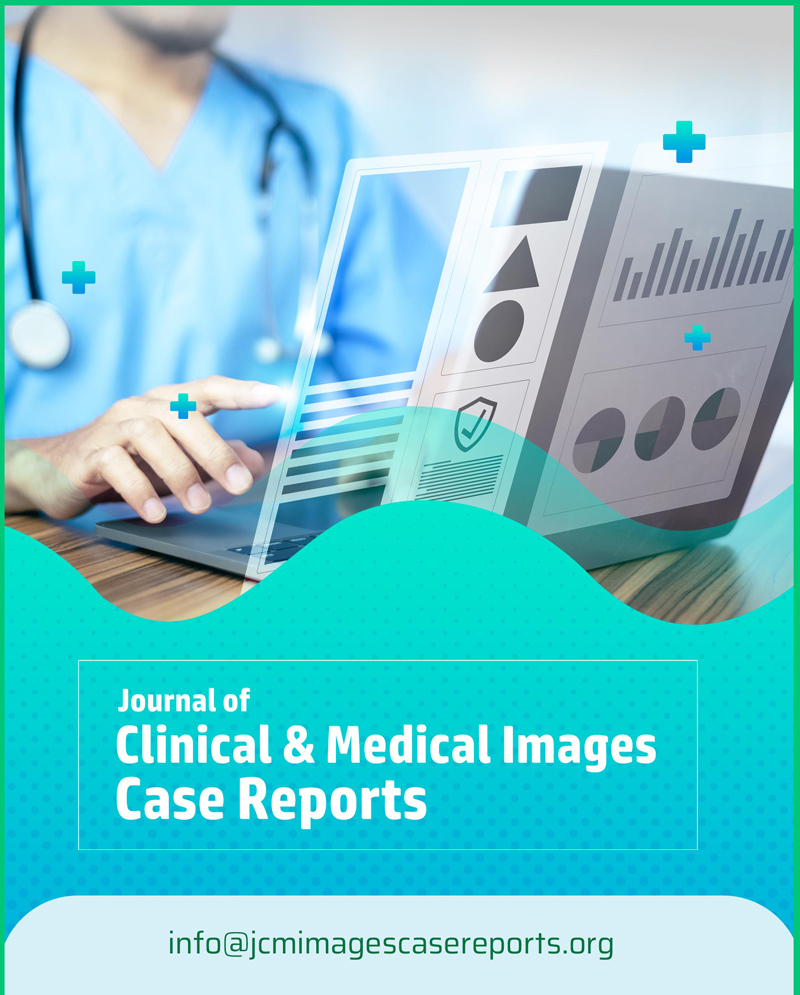
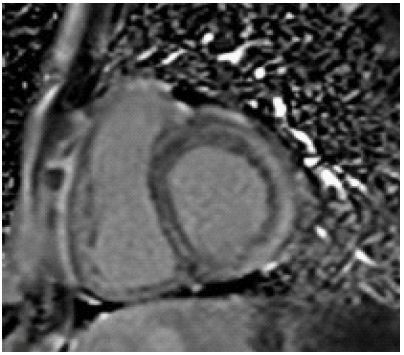
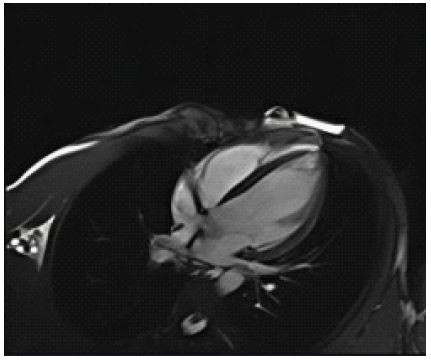
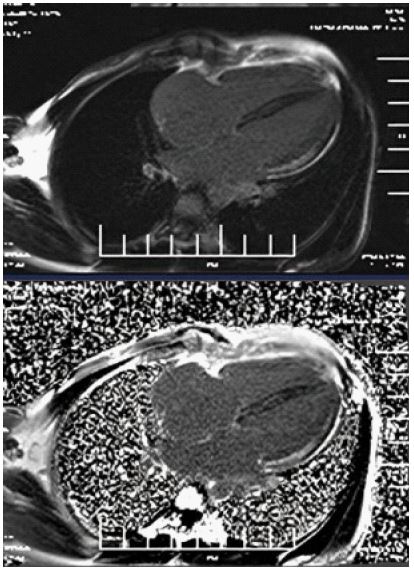
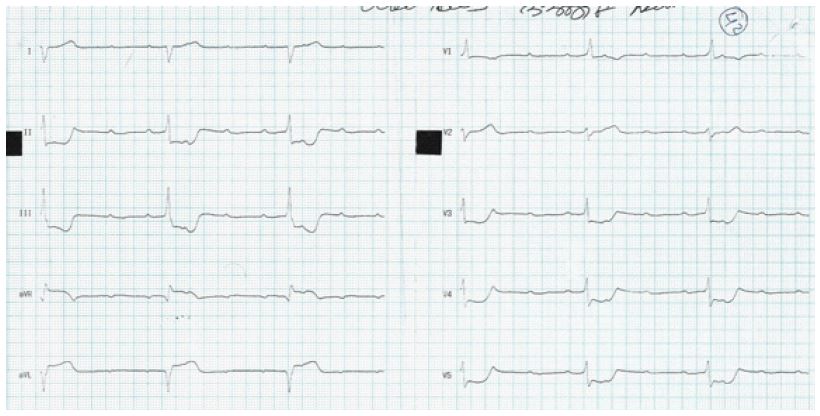
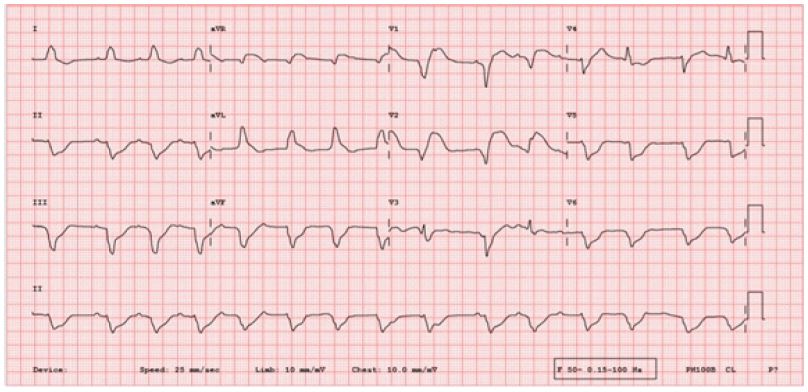
A 33-year-old female with no prior comorbidities presented with a seven-day history of high-grade fever, chills, rigors, dyspnea, and cough with borderline blood pressure requiring inotropes. Preliminary evaluation with ECG revealed sinus tachycardia and a 2D echo revealed global LV hypokinesia and severe Left ventricular dysfunction with LVEF of 30%. Initial laboratory investigations revealed elevated troponin with elevated NT-Pro-BNP suggestive of myocardial injury and acute heart failure, anemia (Hb: 9 g/dL), and elevated TSH (7.8 mIU/L), and mild renal dysfunction. The patient was admitted to the Intensive Care Unit and was treated for Heart Failure. A cardiac MRI was done, and it showed significant mid-myocardial Late Gadolinium Enhancement (LGE) in the LV free wall, sparing the endocardium and epicardium. While mid-myocardial LGE is commonly associated with myocarditis, it can also be seen in other conditions such as sarcoidosis, dilated cardiomyopathy, and Anderson Fabry disease. In this case, the findings were interpreted in conjunction with the clinical presentation, including recent febrile illness, elevated troponin, and rapid LV dysfunction. The imaging met the revised Lake Louise Criteria, supporting a diagnosis of probable myocarditis (Figures 1-3). Patient was started on IV Methylprednisolone 1 g daily for three days and then started on Oral prednisolone 1 mg/kg/day. Four days into her illness, she experienced two syncopal episodes and was found to have bradycardia with a heart rate of 30/min. An ECG revealed a complete heart block (Figure 4) with a wide-complex escape rhythm, and rising troponin levels indicated myocardial injury. A transvenous temporary pacemaker was placed, stabilizing her initially. A formal Transthoracic Echocardiogram (TTE) was performed after temporary pacemaker placement, which revealed the same moderate to severe LV dysfunction and no additional complications. Sarcoidosis was considered due to mildly elevated ACE levels (61 U/L), but further testing, including CT chest, EBUS, and node biopsy, was not feasible due to the patient’s rapid deterioration. Giant cell myocarditis, though rare in young patients, was also considered, given the aggressive course and refractory ventricular arrhythmias. A comprehensive evaluation could not be conducted due to the rapid progression of the disease. However, viral myocarditis remained the most likely etiology based on clinical presentation, negative H1N1 swab, and absence of autoimmune markers (ANA: 1:40, dsDNA < 30 IU/mL) (Table 1). After TPI, she developed slow ventricular tachycardia (130/min) (Figure 5), which persisted despite multiple attempts at overdrive pacing. Amiodarone was initiated (150 mg IV bolus, followed by 1 mg/min for 6 hours, then 0.5 mg/min for 18 hours), but VT remained refractory. Lidocaine (1.5 mg/kg IV bolus, followed by 1 mg/min infusion) was added, but the arrhythmia remained refractory. Overdrive pacing was attempted but was discontinued after the onset of Polymorphic Ventricular Tachycardia (PMVT). Given the fulminant nature of myocarditis, catheter ablation was not attempted, as the arrhythmogenic substrate was likely diffuse rather than focal, reducing the likelihood of procedural success. The patient continued to deteriorate into refractory cardiogenic shock despite maximal inotropic and antiarrhythmic therapy. She experienced cardiac arrest and could not be resuscitated. Referral for mechanical circulatory support (ECMO) was considered, but stabilization for transfer was not possible given the rapid decline. Post-mortem biopsy was not performed due to lack of consent.
| Parameter | Patient value | Normalrange |
|---|---|---|
| Hemoglobin (Hb) | 9 g/dL | 12-16 g/dL |
| Creatinine | 1.5mg/dL | 0.6-1.2 mg/dL |
| TSH | 7.8 mIU/L | 0.4-4.0 mIU/L |
| Troponin I | 1.2ng/mL | <0.04 ng/mL |
| Sodium | 145 mmol/L | 135-145 mmol/L |
| Potassium | 3.2 mmol/L | 3.5-5.0 mmol/L |
| Magnesium | 1.8mg/dL | 1.7-2.2 mg/dL |
| NT-proBNP | 6000 pg/mL | <125 pg/mL |
| Total Bilirubin | 2.1mg/dL | 0.1-1.2 mg/dL |
| Albumin | 5.6g/dL | 3.5-5.0 g/dL |
| ALT | 210 U/L | 10-40 U/L |
| AST | 180 U/L | 10-40 U/L |
| ANA (Titer) | 1:40 | ≤1:40 (negative) |
| Anti-dsDNA | <30 IU/mL | <30 IU/mL (negative) |
| Serum ACE | 61 U/L | 8-52 U/L |
| H1N1 Swab | Negative | Negative |
| Covid 19 | Negative | Negative |
| Parameters | Fulminantmyocarditis | Non-Fulminantmyocarditis |
|---|---|---|
| Onset of Symptoms | Distinctonset of symptoms within 2-4 weeks | Indistinct onset of symptoms |
| Heart failure Symptoms | Class 4often | Class 2-class 4 (variable) |
| Course | Rapidlyprogressive downhill course withoutintervention | Variable without intervention |
| Hypotension inacute stage | Oftenpresent with a needfor inotropes and vasopressors | Maybe present uncommonly |
| Cardiogenic Shock in acute stage | Often present, need for IABP, VAD, VA- ECMO | Not present |
| Arrhythmia | VT andhigh-grade AV blocks are morecommon | Usually,sinus tachycardia, VT, andheart block are less common |
| EMB | Class 1indication | Only neededif LVSD persists. GDMT when asystemic disorder is suspected. |
| Ejection fraction on admission | Severe LVdysfunction is very common | Severe LVSD is not as common in acute stages |
| Need for Heart transplant | More | Not as common as FM |
| In hospital Mortality rate | Higher | Lower |
| Ejection fraction in Long term Follow up | Dramatic improvement but overall EF is lowerthan NFM | Itmay normalize, may be static, but overall EF is higher than FM |
| Indicator | Description |
|---|---|
| I | Inotropes neededfor hemodynamic support |
| N | NYHA ClassIII-IV symptoms |
| E | End-organ dysfunction |
| E | Ejection Fraction severely reduced (<20%) |
| D | Device support escalating (e.g., ICD, CRT) |
| H | Hospitalization for heart failure |
| E | Edema, refractory |
| L | Low blood pressure |
| P | Progressive decline |
| Constraint | Description | Possible Solutions |
|---|---|---|
| Cost of MCS devices | High costs limit availability | Develop cost-effective,portable alternatives |
| Infrastructure | Limited facilitiesfor advanced care | Create regional hubs forspecialized treatment |
| Trained Personnel | Shortage of trainedhealthcare providers | Provide robust training programs and workshops |
| Diagnostic Tools | Lack of advancedimaging like MRI and biopsy | Focuson clinical and basicdiagnostic parameters |
| Referral Pathways | Delayed recognition andtransfer | Develop structured referral networks |
Fulminant myocarditis is a severe manifestation of myocarditis, characterized by rapid hemodynamic decline necessitating aggressive intervention. Lieberman et al. (1991) first described fulminant myocarditis by its acute symptom onset, histological evidence of multiple foci of active myocarditis, and a binary outcome of complete recovery or death. (2) However, this definition, reliant on Endomyocardial Biopsy (EMB), initially excluded eosinophilic and giant cell myocarditis, leading to underreporting. Updated criteria proposed by Ammirati et al. (2017) include acute symptom onset within 2-4 weeks, hemodynamic instability, and the need for MCS [3]. Fulminant myocarditis often remains underdiagnosed due to its rapid progression. Autopsy studies reveal myocarditis to be a significant cause of sudden cardiac death, especially in young individuals. Fulminant myocarditis differs with respect to garden variety myocarditis due to abrupt symptom onset, severe left ventricular dysfunction, cardiogenic shock, and life-threatening arrhythmias such as ventricular tachycardia or heart block. Non-fulminant myocarditis progresses more gradually with milder symptoms. Survivors of fulminant myocarditis may experience dramatic left ventricular function recovery, although long-term ejection fraction remains lower compared to non-fulminant cases (Table 2) [4-6].
Fulminant myocarditis can arise from various etiologies, broadly classified into viral, autoimmune, toxic, infiltrative, and bacterial causes. Viral myocarditis remains the most common, with Coxsackievirus, Parvovirus B19, Influenza (H1N1), and Adenovirus frequently implicated. Autoimmune and inflammatory causes include Systemic Lupus Erythematosus (SLE), sarcoidosis, giant cell myocarditis, and eosinophilic myocarditis. Toxic myocarditis may result from drug-induced injury (e.g., anthracyclines, checkpoint inhibitors, cocaine) or hypersensitivity reactions. Infiltrative myocarditis, such as sarcoidosis, amyloidosis, and Anderson-Fabry disease, can lead to chronic myocardial dysfunction. Bacterial and other infectious causes, including Lyme disease, Chagas disease, and diphtheria, are less common but remain important considerations in endemic regions [7]. Management of fulminant myocarditis requires early and aggressive intervention. Recognizing fulminant myocarditis and early referral to advanced centers is critical for improving outcomes. In our case, several clinical findings necessitated early referral, such as persistent hypotension despite initial stabilization efforts and escalating NT-proBNP levels (6000 pg/mL), indicating severe myocardial stress, Complete heart block, and subsequent refractory ventricular arrhythmias, including polymorphic VT. These parameters align with the “I-NEED-HELP” mnemonic (Table 3) and underscore the need for early MCS therapy. MCS, such as VA-ECMO or LVAD, plays a pivotal role in bridging patients through the acute phase or to transplantation [8,9]. Outcomes in cardiac conditions vary significantly based on etiology and access to advanced care. Although in-hospital mortality remains high, survivors often demonstrate significant recovery of left ventricular function, particularly during the initial weeks after onset. Despite this, barriers such as the high cost of Mechanical Circulatory Support (MCS) devices, limited availability of trained personnel, and inadequate infrastructure pose significant challenges. To address these issues, initiatives could focus on developing cost-effective MCS alternatives, such as portable or simplified ECMO systems, and implementing robust training programs for healthcare professionals. Additionally, establishing regional hubs equipped with advanced resources and fostering international collaborations could improve accessibility and outcomes in underserved areas (Table 4). Routine heart failure therapies should be initiated after stabilization, following guideline-directed medical therapy. Incorporating structured referral criteria and practical advice for resource-limited settings can significantly improve early detection and management. Establishing standardized protocols based on accessible clinical signs and tools, such as reliance on echocardiography and ECG findings, can bridge the gap where advanced diagnostics are unavailable [10].
Fulminant myocarditis is a medical emergency requiring rapid diagnosis and aggressive management. Mechanical circulatory support, especially VA-ECMO, has become a vital therapeutic option. Despite significant advancements, fulminant myocarditis remains associated with high mortality and long-term morbidity, emphasizing the need for continued research and early intervention strategies.